Thyroid nodules
- related: Endocrinology
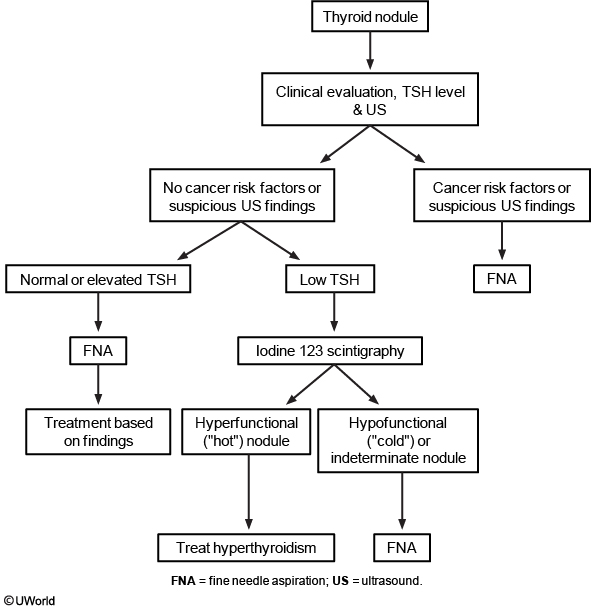
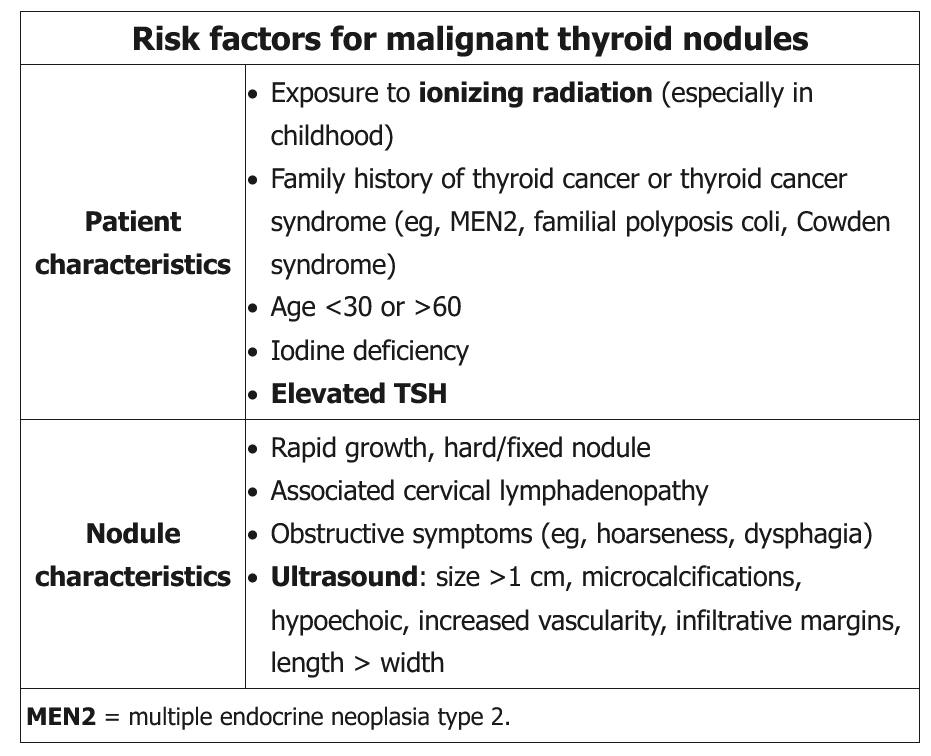
Patients with thyroid nodules >1 cm should be evaluated based on their cancer risk factors (eg, family history, past radiation exposure, cervical lymphadenopathy), compressive symptoms (eg, hoarseness, difficulty swallowing), and thyroid functional status (ie, euthyroid, hyperthyroid, or hypothyroid). In general, an ultrasound of the thyroid should be obtained first. Patients with suspicious ultrasound findings (eg, hypoechoic, microcalcifications, internal vascularity) or cancer risk factors should undergo fine-needle aspiration (FNA). Measurement of serum TSH can further stratify the risk of malignancy in patients with a thyroid nodule. Patients with normal or elevated TSH levels have a higher risk of malignancy and should be evaluated with FNA.
Patients with low TSH levels should be evaluated using thyroid scintigraphy, usually with iodine 123. A hyperfunctioning (“hot”) nodule (increased isotope uptake in the nodule with decreased surrounding uptake) is rarely malignant and may be treated as benign hyperthyroidism. An indeterminate or hypofunctioning (“cold”) nodule indicates a higher risk of cancer and requires further evaluation with FNA.
Hypofunctioning (“cold”) or indeterminate nodules have a higher malignancy risk and may require FNA based on size, ultrasound findings, and patient characteristics:
- High-risk findings on ultrasound include microcalcifications, increased vascularity, hypoechoic appearance, elongated shape, and indistinct or irregular nodule margins. FNA is indicated in such nodules ≥1 cm.
- Low-risk nodules on ultrasound (eg, isoechoic, hyperechoic, partially cystic, spongiform) are monitored and biopsied if they grow to ≥1.5-2 cm.
- Purely cystic nodules are almost always benign and do not require FNA.
- High-risk patient characteristics include a personal or first-degree family history of thyroid cancer, history of radiation exposure in childhood, rapid nodule growth, and cervical lymphadenopathy. FNA should be considered for any size of nodule in this population.
This patient has a painless thyroid nodule without clinical risk factors for thyroid cancer, compressive symptoms, or features suggesting hyperor hypothyroidism. However, due to the size of the nodule and normal TSH level, this patient should have FNA to rule out malignancy.