13 Electrolytes
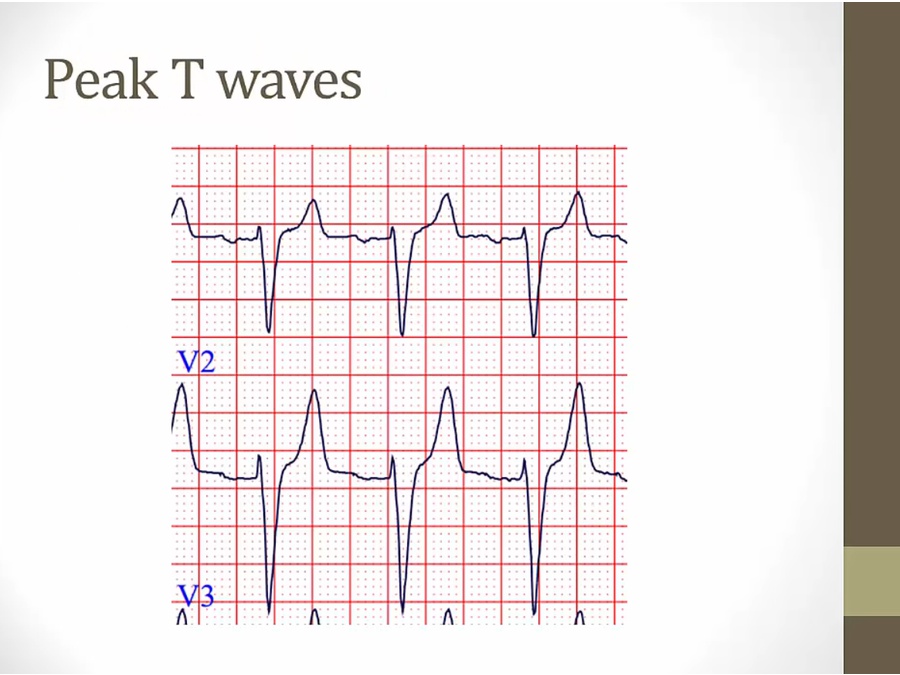
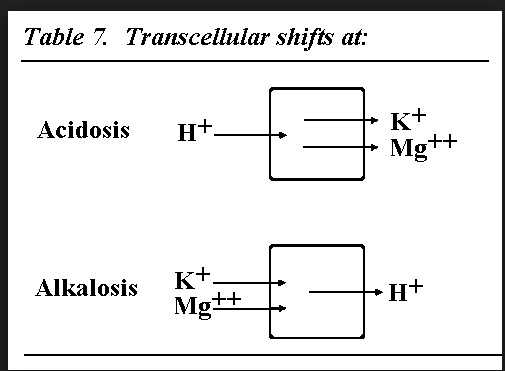
- hyperkalemia: wide QRS, peaked T, weakness
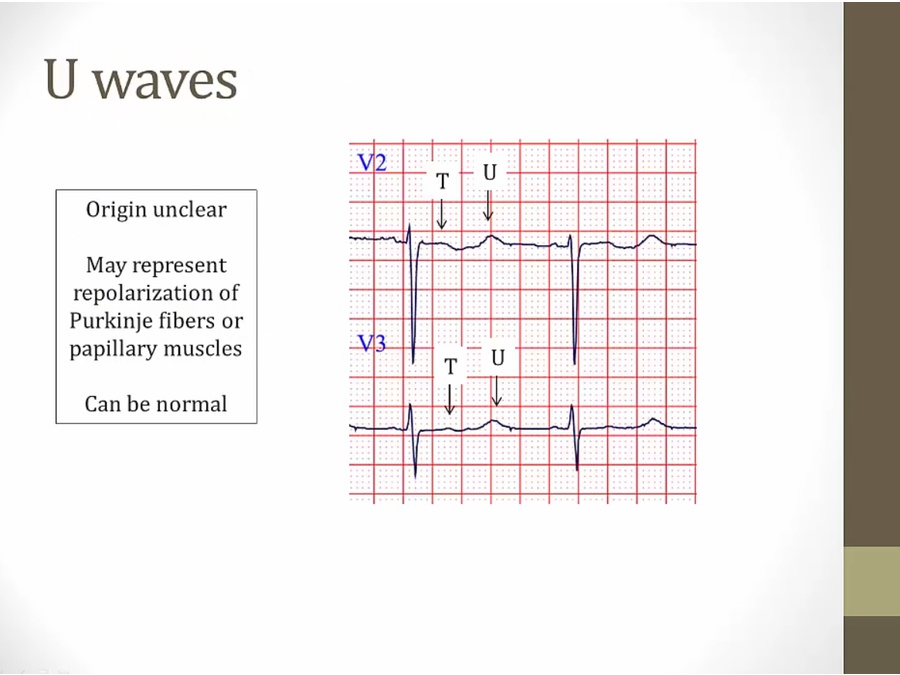
- hypokalemia: flat T, U wave, weakness
- hypercalcemia: stones, bones, groans, psychiatric overtones
- hypocalcemia: tetany, seizures
- hypermag: decreased DTR, paralysis, bradycardia, hypotension
- hypomag: tetany, arrhythmia, confusion
Hyperkalemia
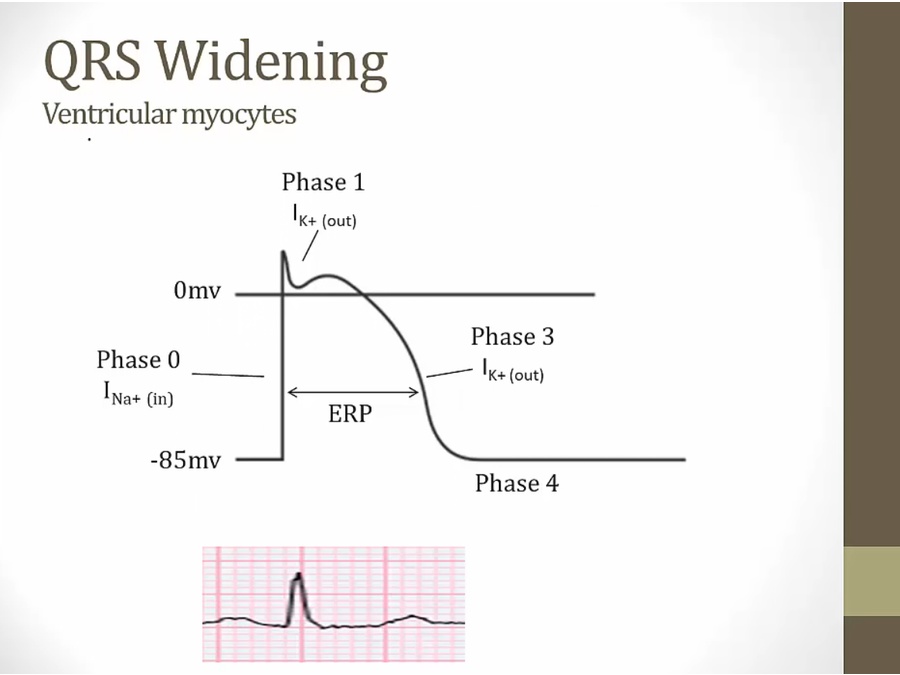
- hyperkalemia: Na channels inactivated, slowing depolarization
Reversal potential of K is shifted positive. Driving force for K to leave the cell via Leak K channels is decreased so there is less “leak” K current and the RMP is depolarized compared to normal. The more positive RMP means more Na channels will randomly open and more of them will become inactivated. This means fewer Na channels are available to respond by opening when full depolarization occurs.
- insulin deficient, beta blockers, digoxin: Na/K pump
- insulin and catecholamines stimulates pump (insulin deficient and bb increase K)
- hyperosmolarity: uncontrolled hyperglycemia

- Banana peels: beta-2 activation can cause hypokalemia (due to increased insulin activity)
- rhabdomyolysis: lysis of cells, hyperkalemia
- hyperosmolar state: draw water out of cell, take K with it, create high K gradient in cell that leaves
Hypokalemia
Hypercalcemia
- promotes water loss and nausea: dehydrated

- mets to bones increase turnover
Hypocalcemia
Hyperphosphatemia
- metastatic calcification: end stage renal pts with high phosphate
- phosphate laxatives: bowel prep for GI exam
Hypophosphatemia
- ammonia binds phosphate
- tumor: inhibit transporter in PCT, don’t resorb phosphate
Hypermagnesemia
- important cause
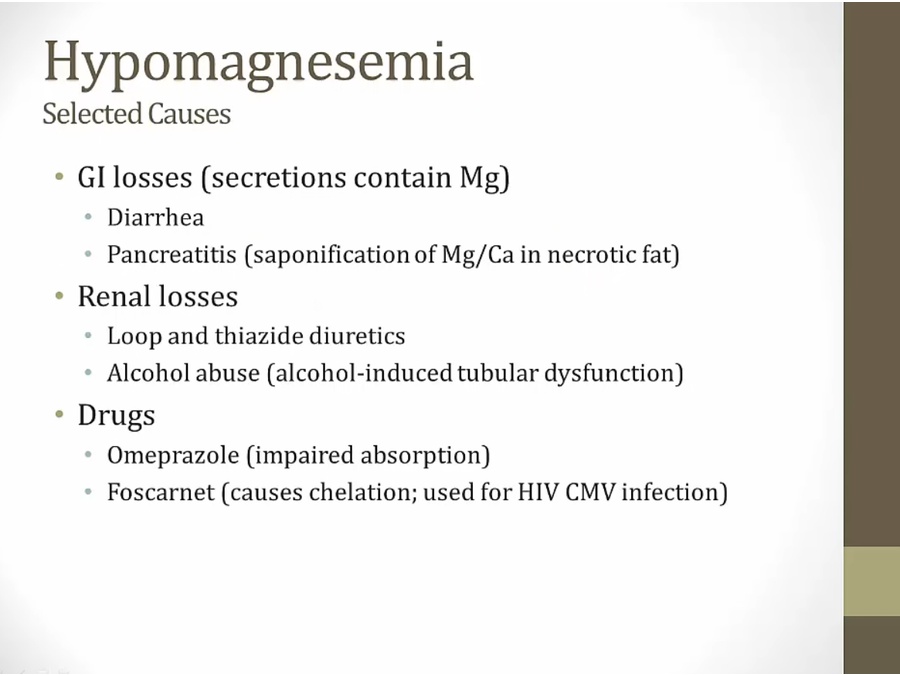
Hypomagnesemia
- drags K and Ca with it