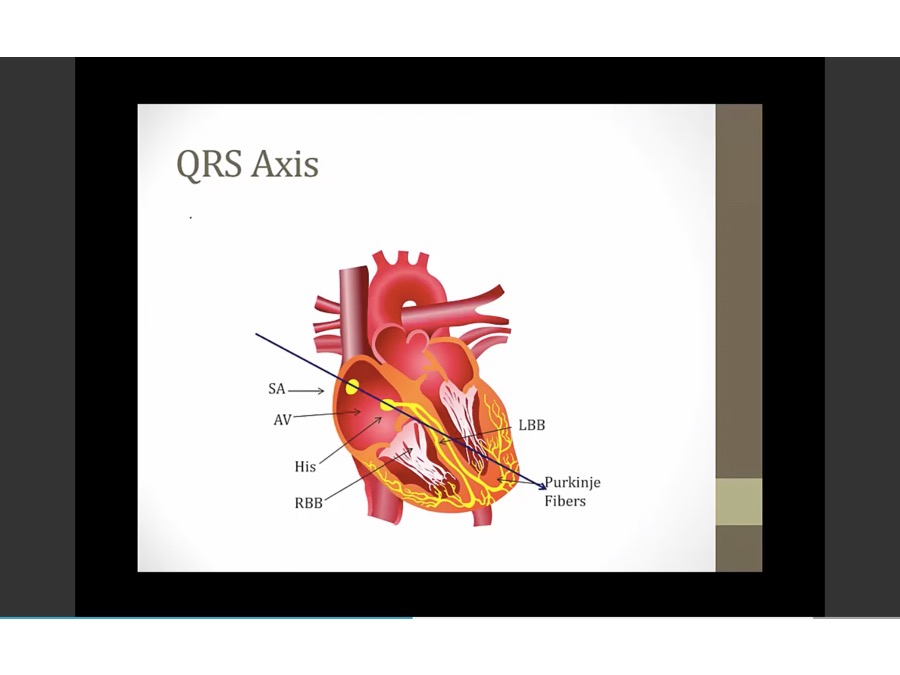
14 EKG Basics
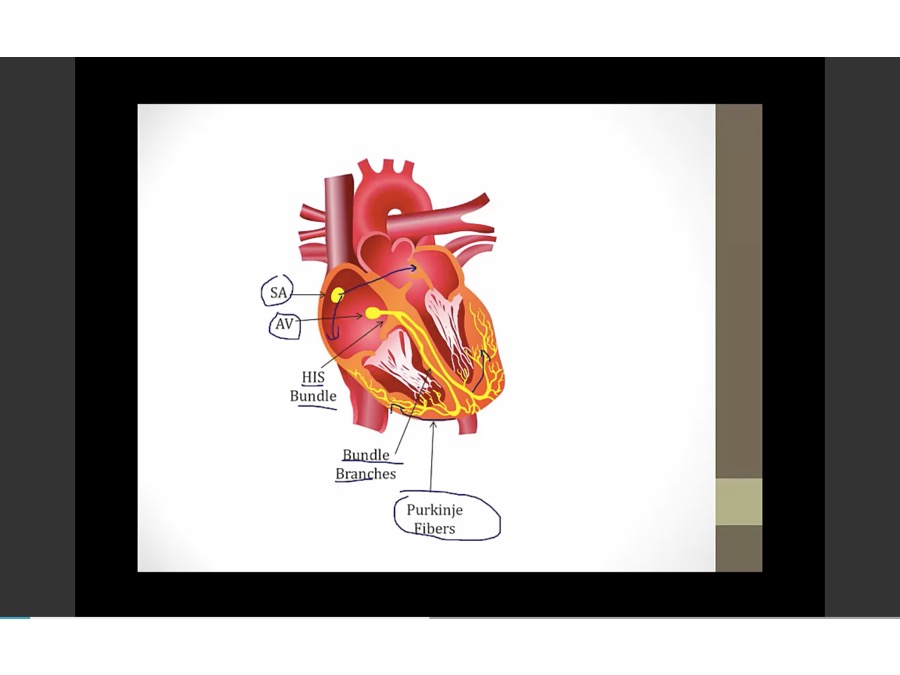
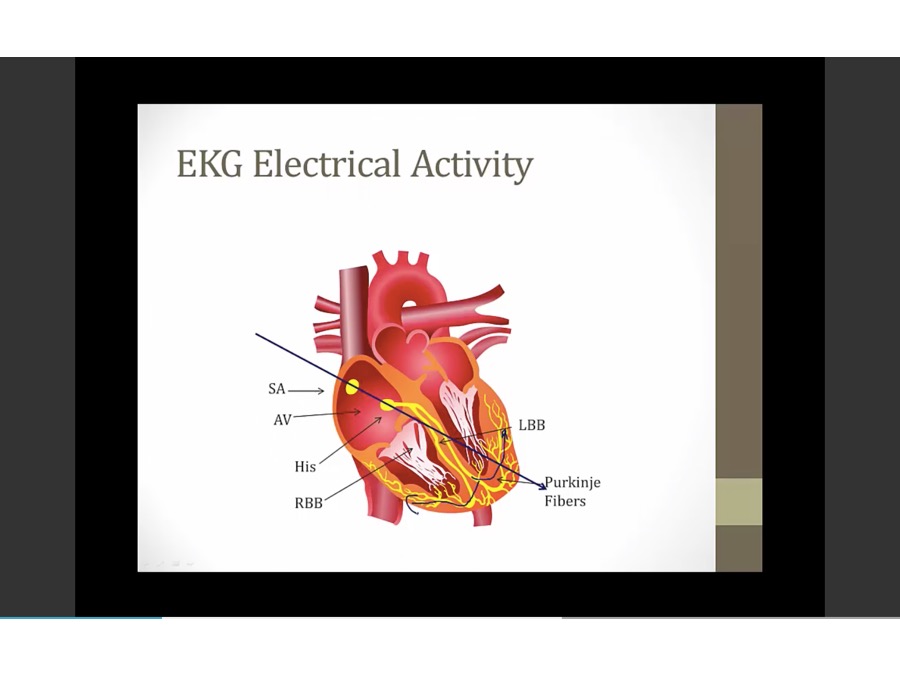
- SA to LA and RA myocytes
- HIS bundles, left and right BBB, purkinje embedded in myocytes
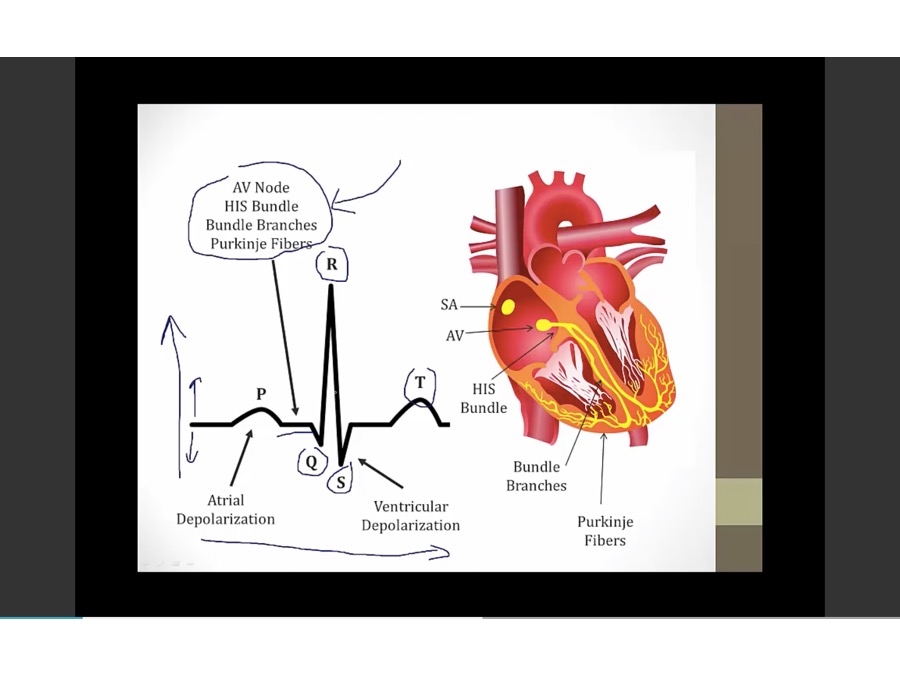
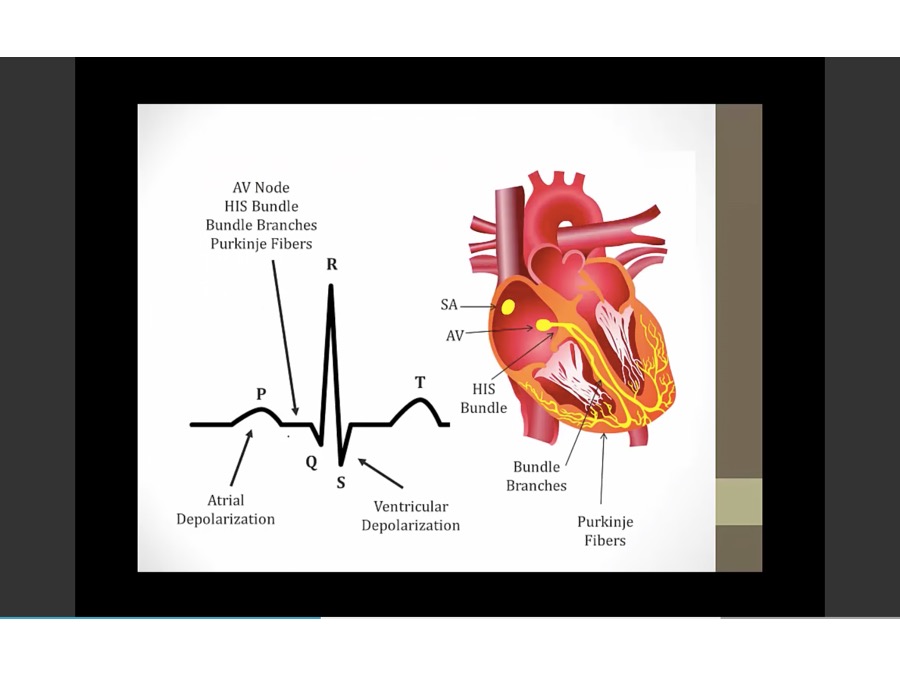
- time x axis, electrical activity in y axis
- P: atrial depolarization
- flat after P: time for electrical activity to go to ventricles
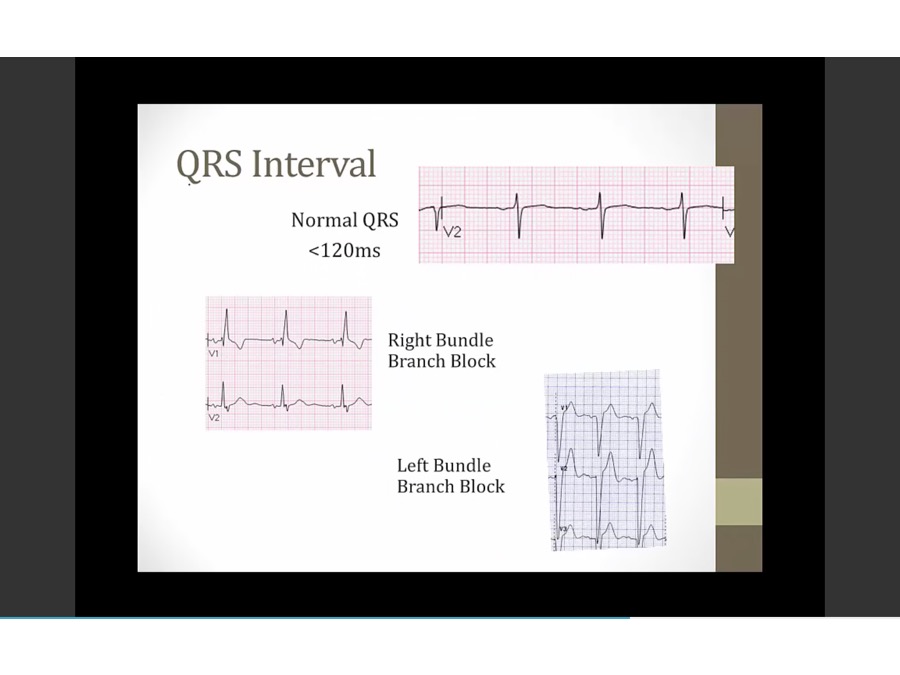
- QRS: ventricle depolarize
- T: repolarization of ventricle. Atrial repolarization happens during QRS
Pacemaker and Hr
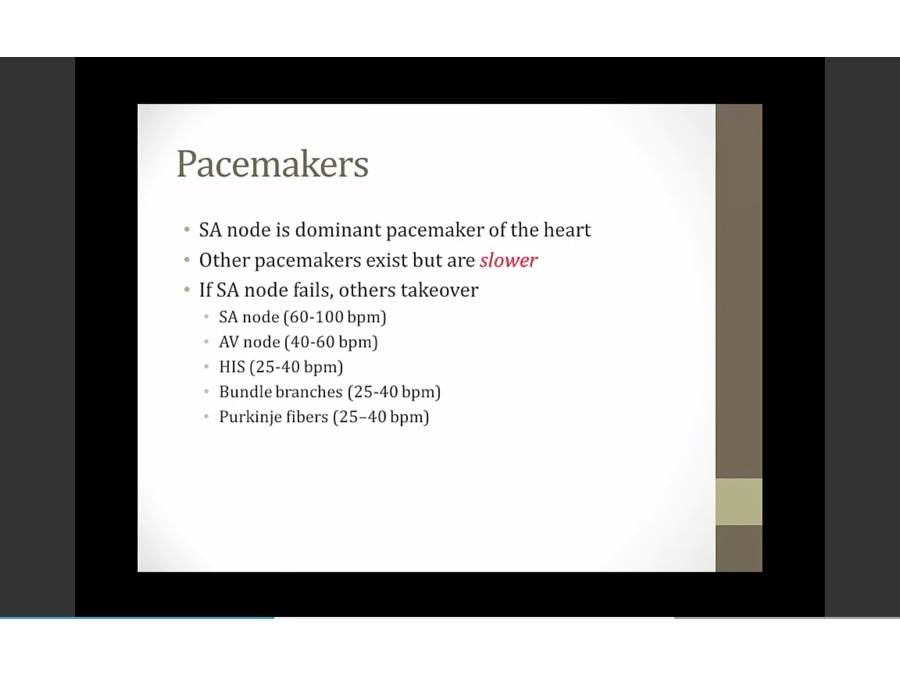
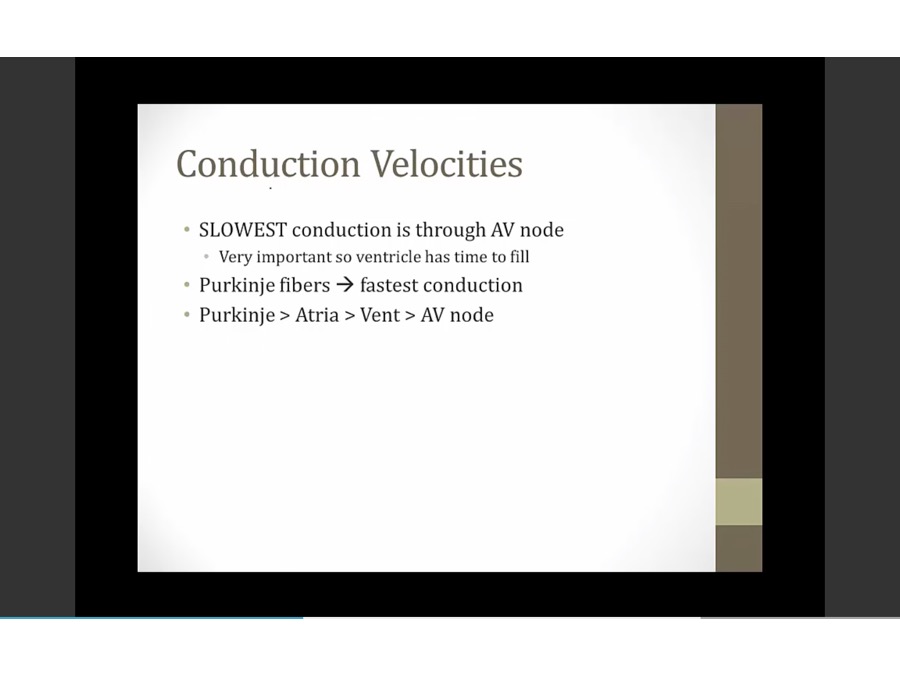
- speed by which electricity moves through heart
- most of time between P and QRS is by AV nodal conduction
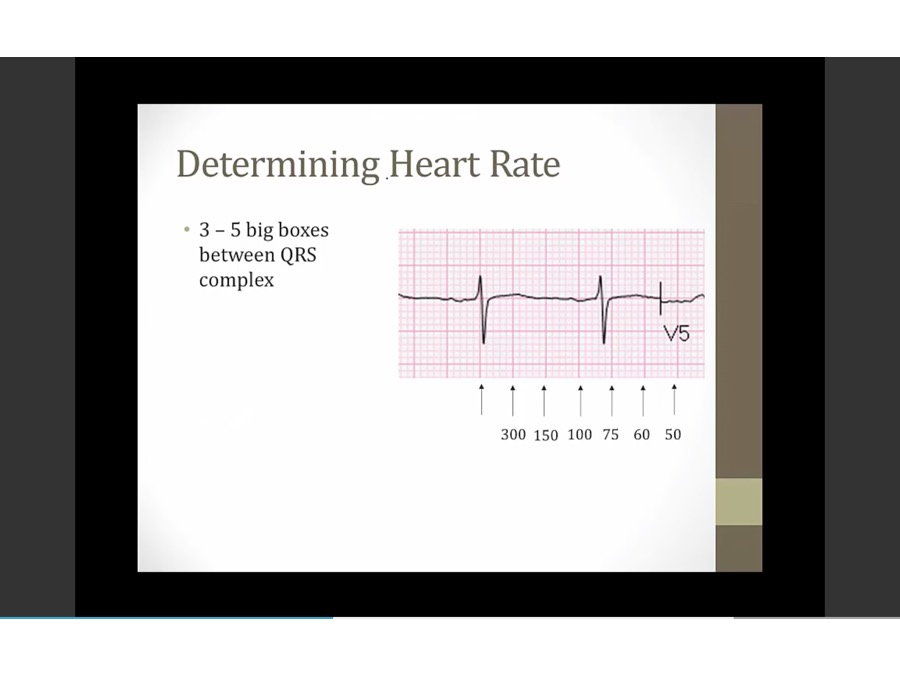
- small box: 40 ms
- big box: 200 ms
- 300 / # of big boxes
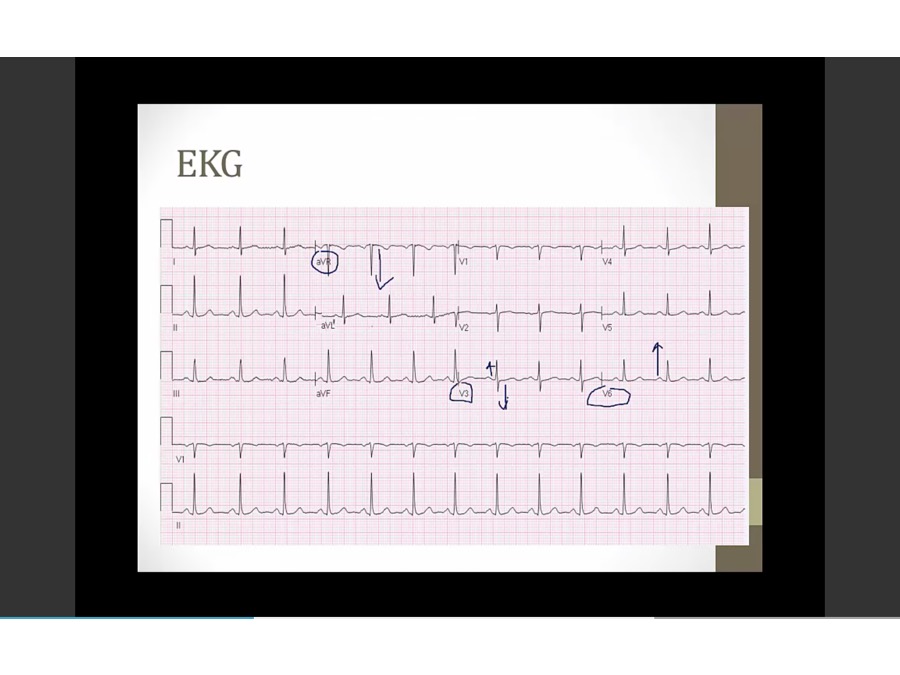
EKG lead
- some electrical activity to left, right
- sum of all activity: arrow
- each of 12 EKG leads look at summation from different POV = different QRS shape
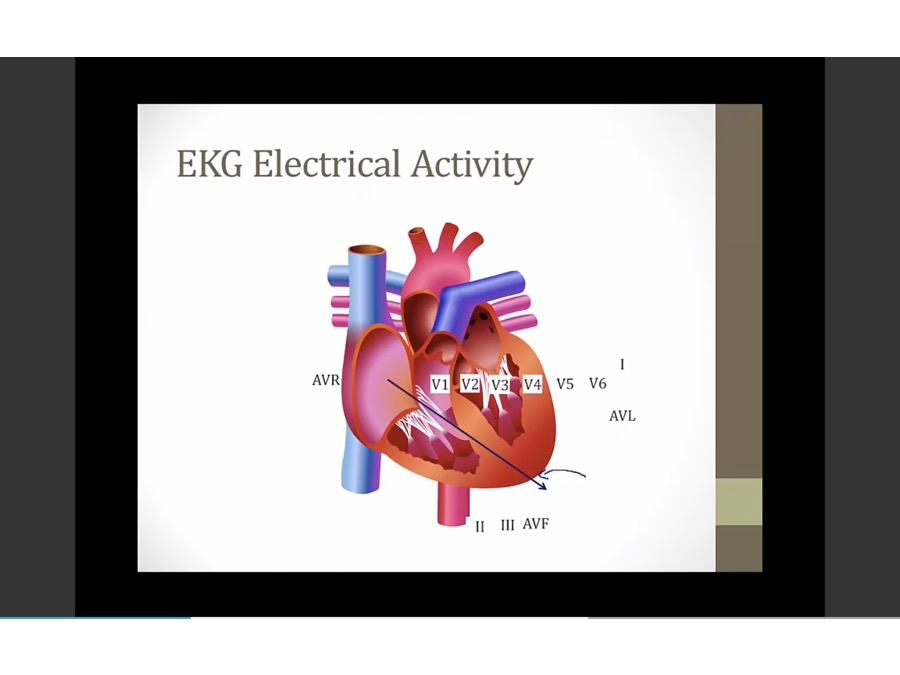
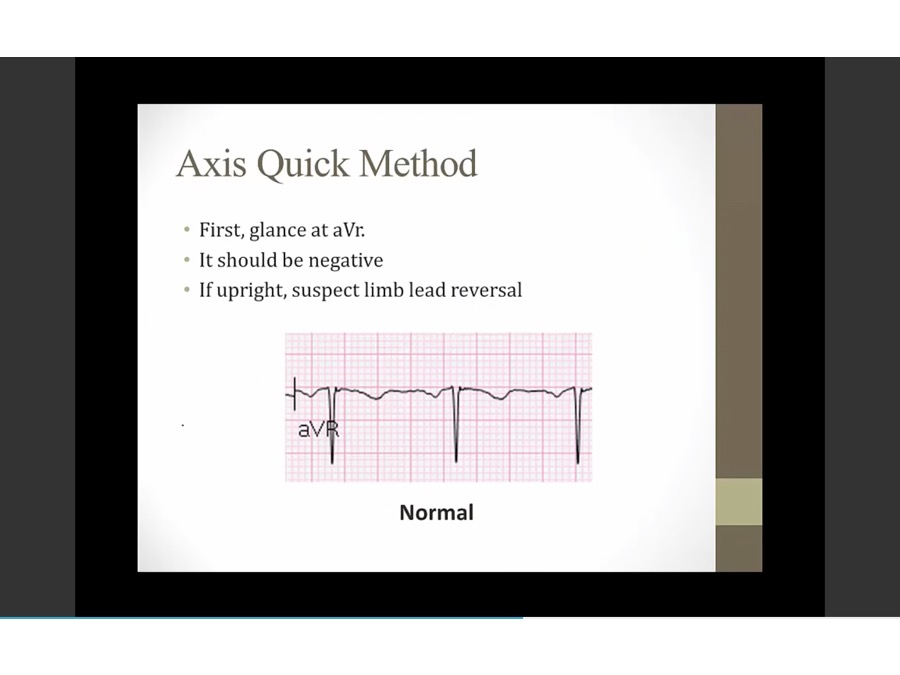
- AVR: summation away, negative QRS
- 1, AVL: summation towards, positive
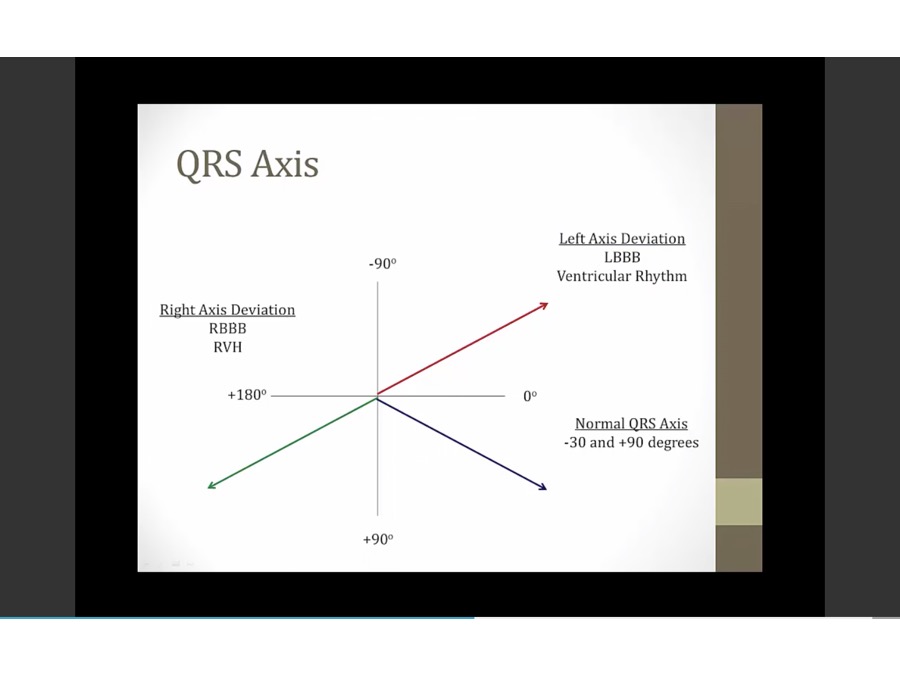
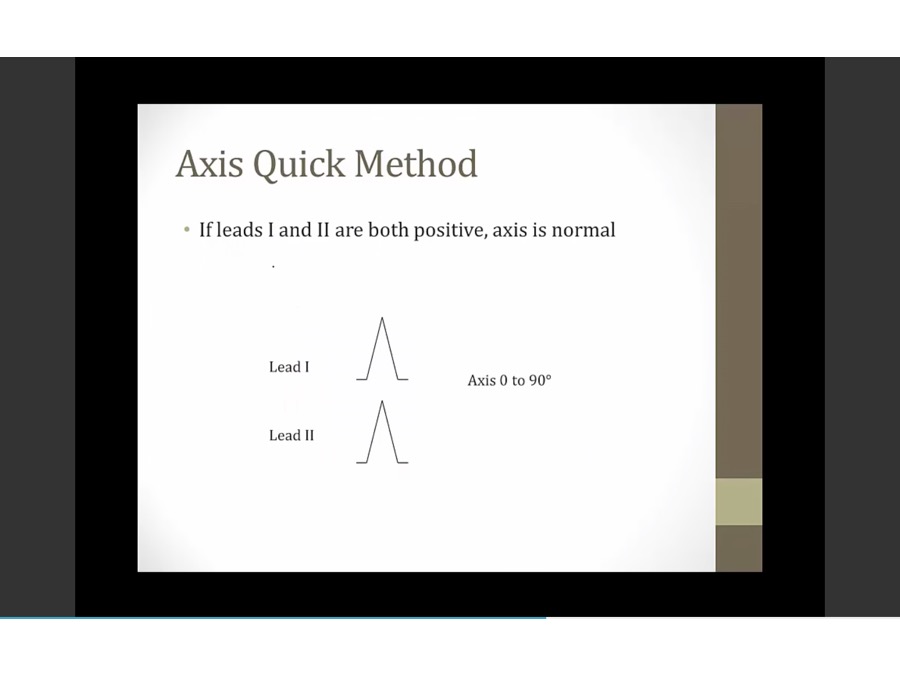
QRS Axis
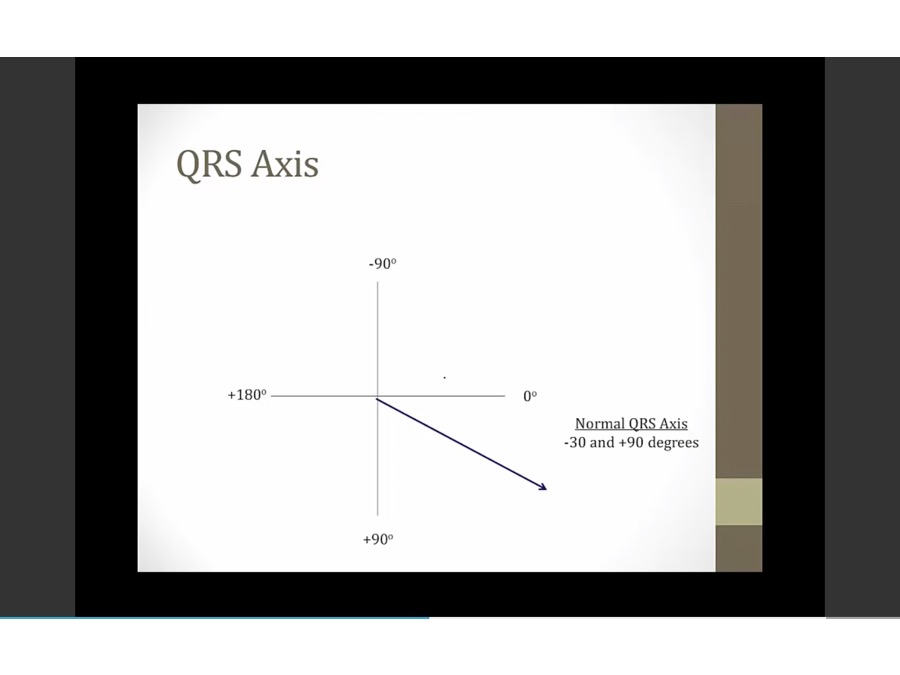
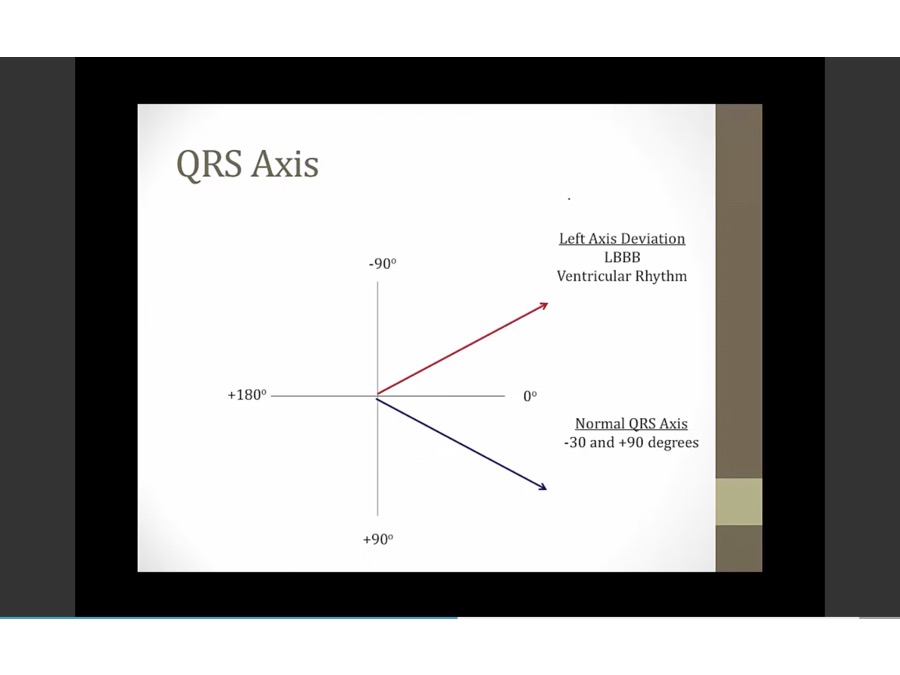
- -30 and -90
- V tach, activity not from SA node but from ventricle itself
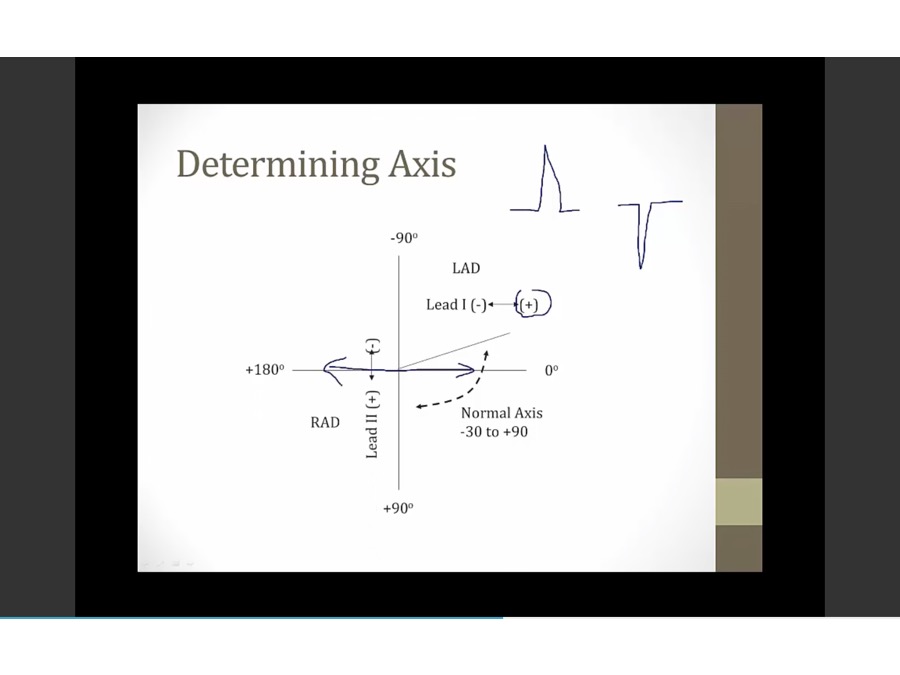
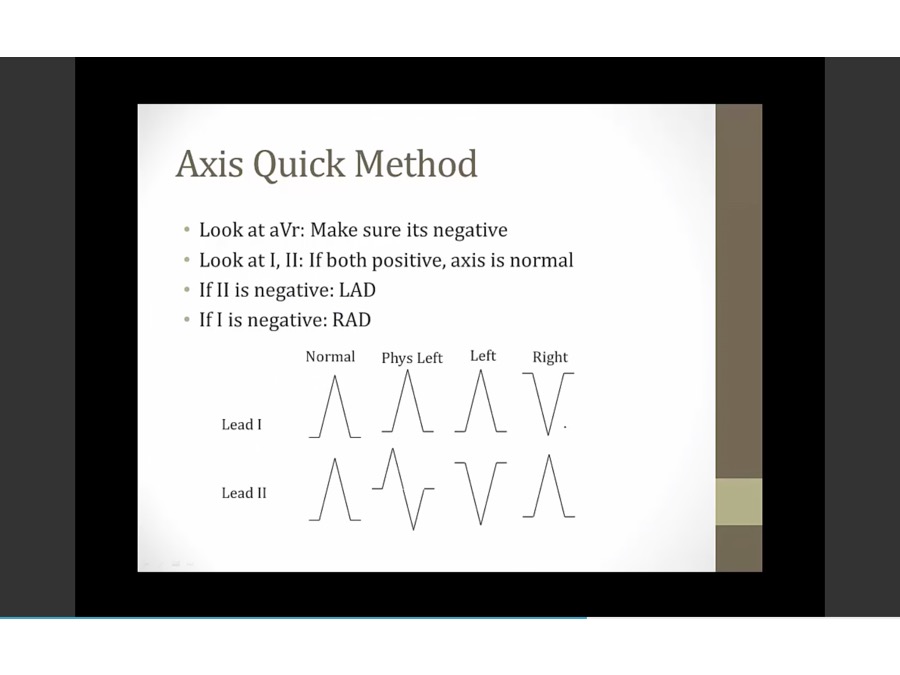
- positive lead 1: toward 0
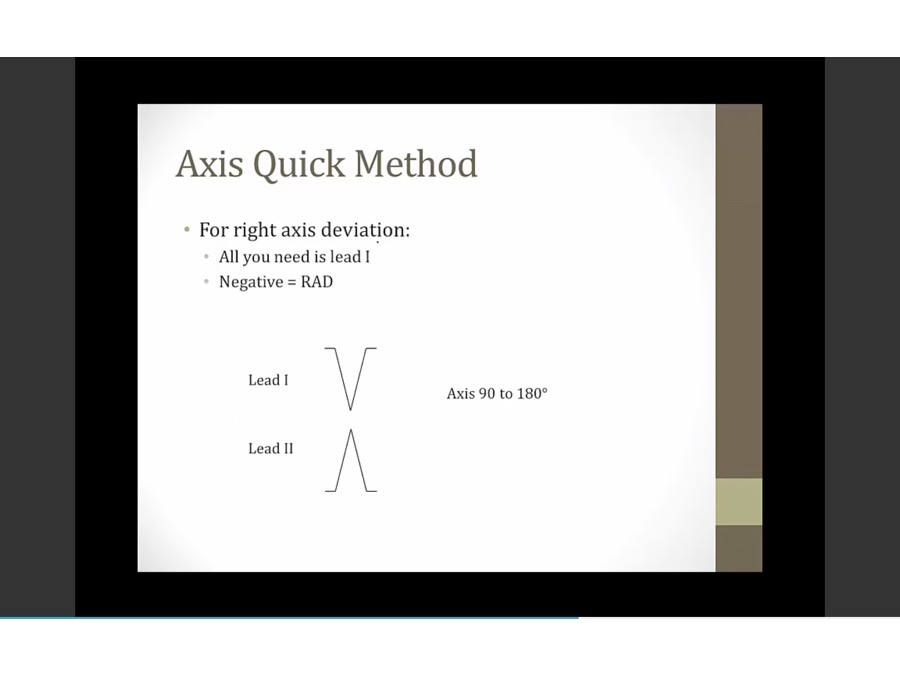
- negative lead 1: towards 180
- positive lead 2: going down
- negative lead 2: going up
- added lead 1 and 2 vectors to have summation vector
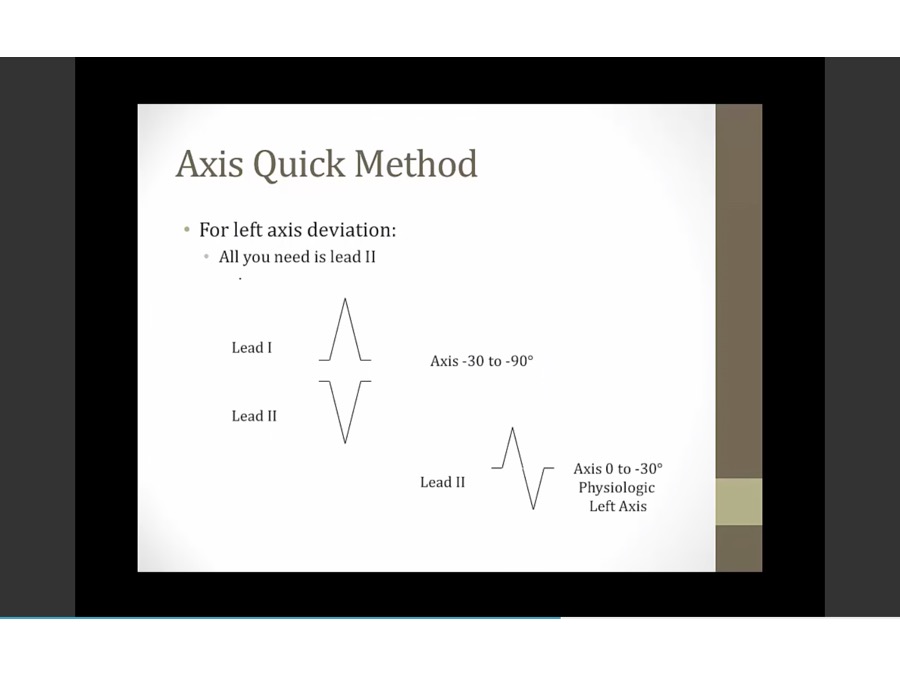
- exception: part up part down, physiologic, slightly to left, nl
Intervals
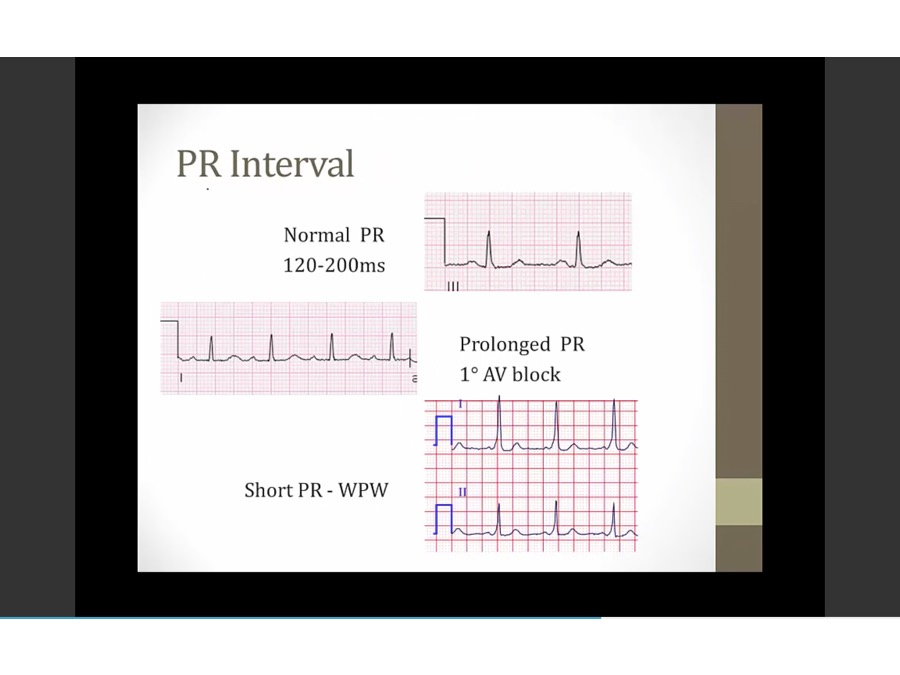
- PR: shorter than 1 big box

- Inactivated peanut butter jar: TCAs block the cardiac fast Na+ channels, decreased contractility, QRS, QT propagation
- Wide QRS crack: TCAs can widen the QRS complex on ECG
- Twisted torsades streamer: TCAs can induce torsades

- Lightly held peanut butter jar: class IA antiarrhythmics have an intermediate binding affinity for the Na+ channel (intermediate use-dependence, moderate slowing of the phase 0 upstroke)
- Pushing away the curtain: class IA antiarrhythmics also block K+ channels, prolonging phase 2 and 3 of the cardiac action potential -> prolonged refractory period
- Twisted torsades streamer: class IA antiarrhythmics can cause Q-T interval prolongation (precipitates torsades) (K channel prolongation)
- Wide QRS shaped crack: class I antiarrhythmics widen the QRS complex on the ECG (decreased AP conduction velocity) (faster cells bind more and slow down more) (QRS widen as HR increases)
- less than half QRS - QRS
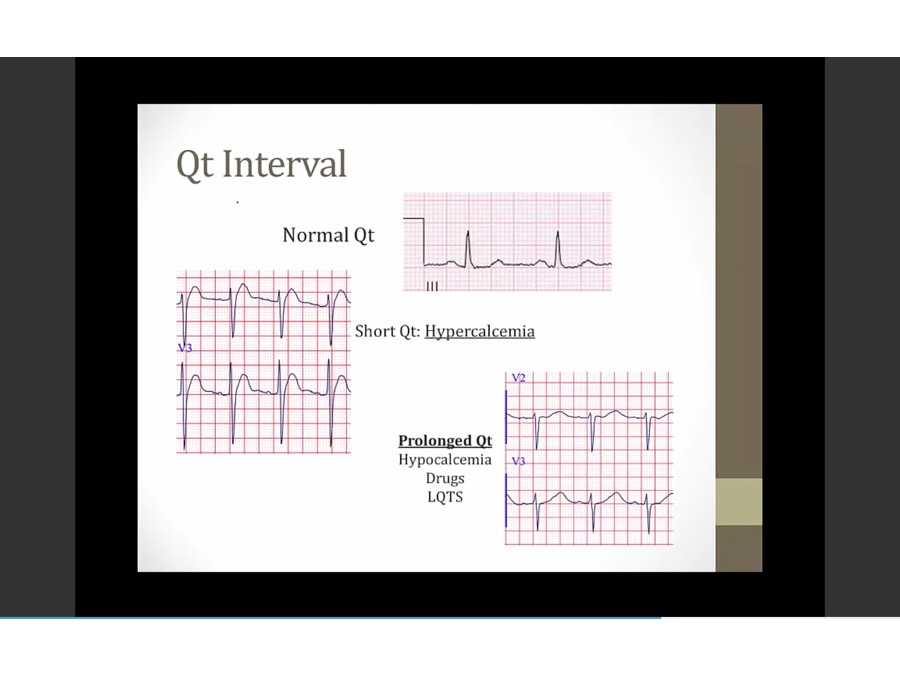
- left: T begin immediately without flat portion
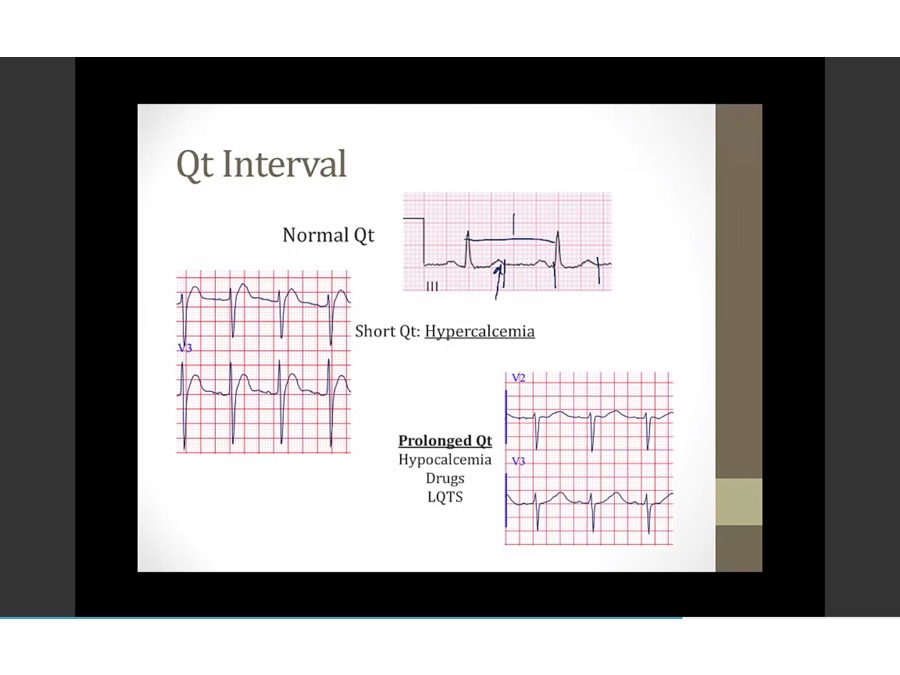
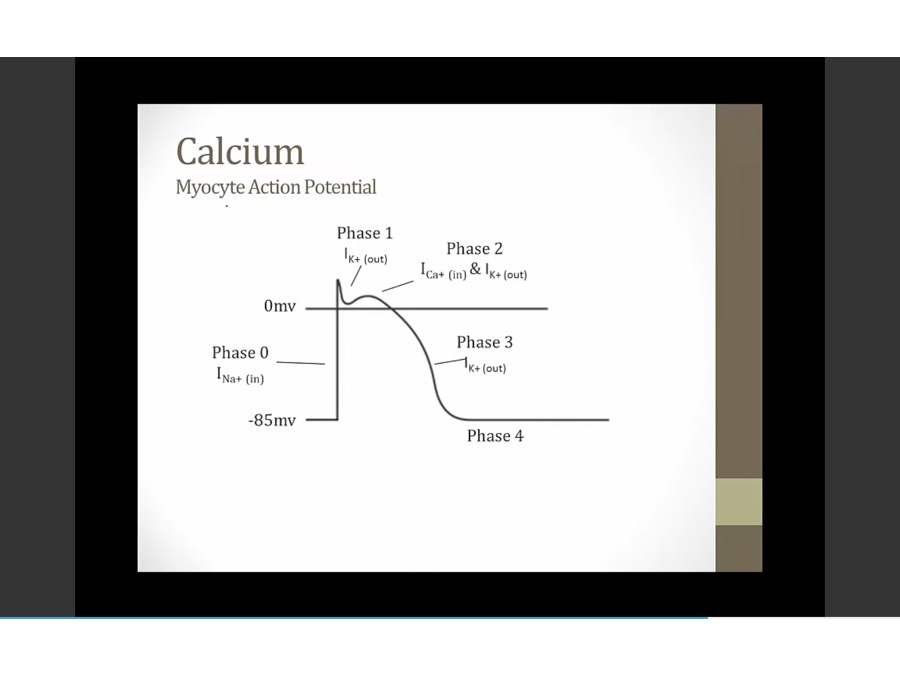
- hypocalcemia: less driving force to move Ca in, longer for Ca to go in, longer for QT interval to occur (myocyte in ventricles to depolarize, repolarize )

- Torsades strip: risk of prolonged Q-T interval


- Twisted streamer: FGAs can cause torsades de pointes
- Lightly held peanut butter jar: class IA antiarrhythmics have an intermediate binding affinity for the Na+ channel (intermediate use-dependence, moderate slowing of the phase 0 upstroke)
- Pushing away the curtain: class IA antiarrhythmics also block K+ channels, prolonging phase 2 and 3 of the cardiac action potential -> prolonged refractory period
- Twisted torsades streamer: class IA antiarrhythmics can cause Q-T interval prolongation (precipitates torsades) (K channel prolongation)
- Wide QRS shaped crack: class I antiarrhythmics widen the QRS complex on the ECG (decreased AP conduction velocity) (faster cells bind more and slow down more) (QRS widen as HR increases)

- Pushing away the curtain: class III antiarrhythmics block K+ channels prolonging phase 2 and 3 of the cardiac action potential -> prolonged refractory period
- Twisted streamer: sotalol, dofetilide, and ibutilide can induce torsades (although all type III antiarrhythmics can widen the QT interval)
- Inactivated peanut butter jar: TCAs block the cardiac fast Na+ channels, decreased contractility, QRS, QT propagation
- Wide QRS crack: TCAs can widen the QRS complex on ECG
- Twisted torsades streamer: TCAs can induce torsades
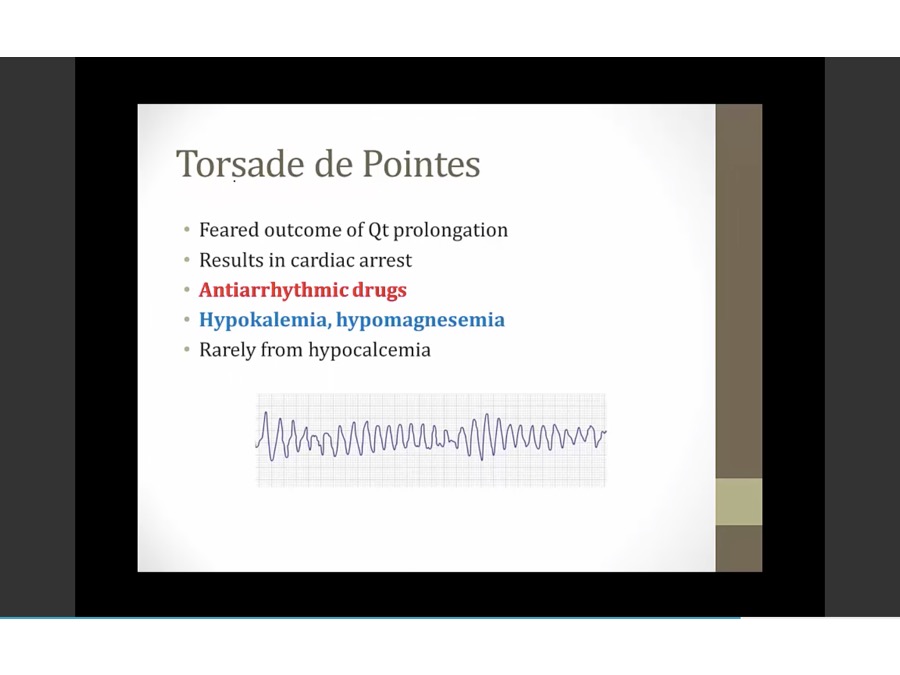
- Torsades strip: risk of prolonged Q-T interval
- Twisted streamer: FGAs can cause torsades de pointes
- Lightly held peanut butter jar: class IA antiarrhythmics have an intermediate binding affinity for the Na+ channel (intermediate use-dependence, moderate slowing of the phase 0 upstroke)
- Pushing away the curtain: class IA antiarrhythmics also block K+ channels, prolonging phase 2 and 3 of the cardiac action potential -> prolonged refractory period
- Twisted torsades streamer: class IA antiarrhythmics can cause Q-T interval prolongation (precipitates torsades) (K channel prolongation)
- Pushing away the curtain: class III antiarrhythmics block K+ channels prolonging phase 2 and 3 of the cardiac action potential -> prolonged refractory period
- Twisted streamer: sotalol, dofetilide, and ibutilide can induce torsades (although all type III antiarrhythmics can widen the QT interval)
- Inactivated peanut butter jar: TCAs block the cardiac fast Na+ channels, decreased contractility, QRS, QT propagation
- Wide QRS crack: TCAs can widen the QRS complex on ECG
- Twisted torsades streamer: TCAs can induce torsades
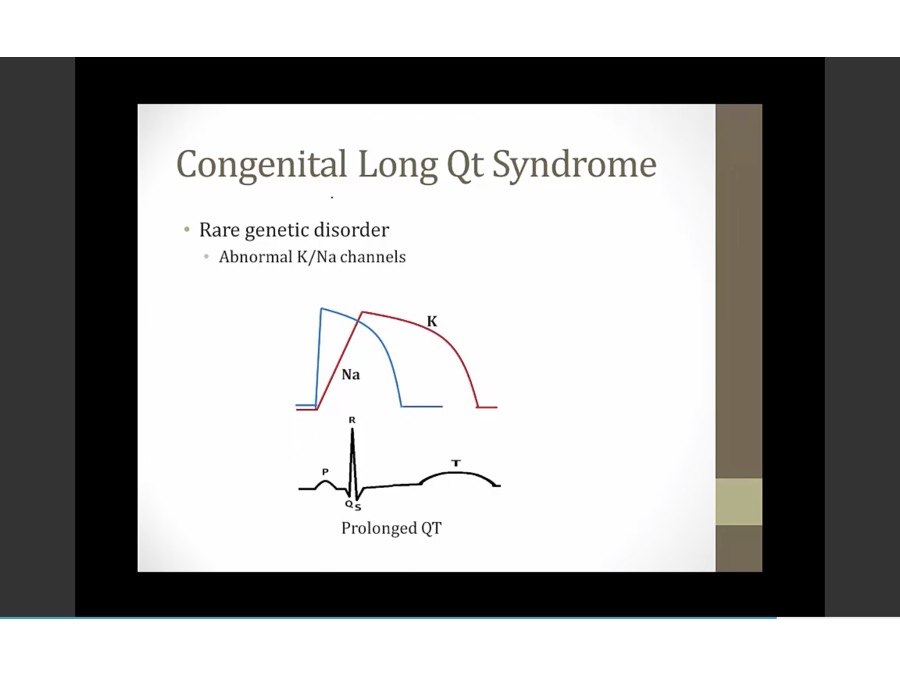
- longer to depolarize/repolarize, longer QT
- not really seizures, passing out from torsades
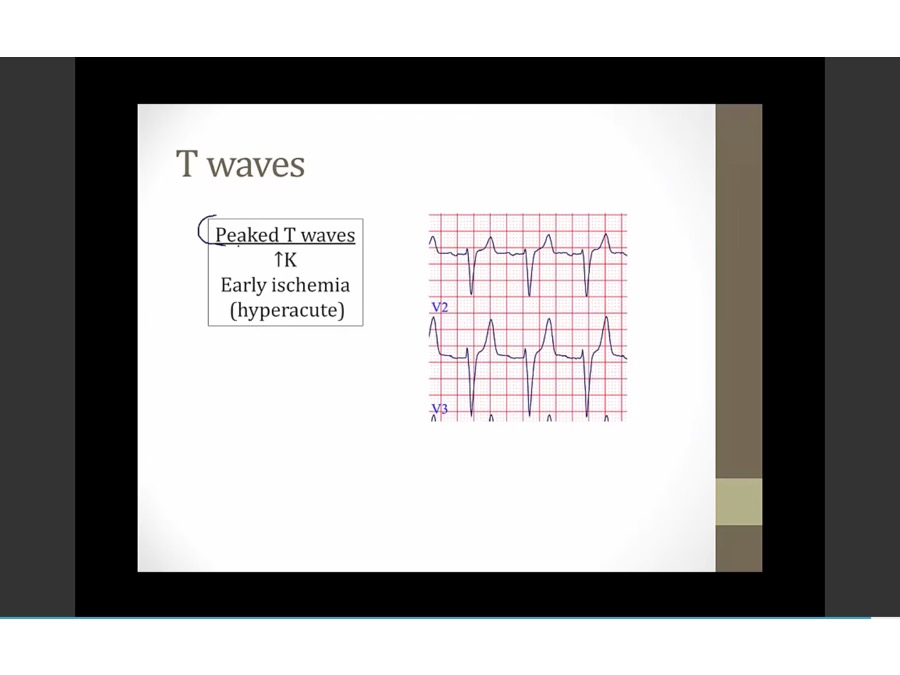
- hyperacute: precede ST elevation in ischemia
Links to this note