14 Na and Water
- Abnormal water balance as result of abnormal ADH: hypo/hypernatremia (SIADH, diabetes insipidus)
- Abnormal Na balance result of abnormal RAAS/SNS: hypo/hypervolemia (HF, hemorrhage)
Effective Circulating Volume
- increase volume, usually increase ECV
- increase CO, increase ECV
- resistance: low resistance, low ECV
_
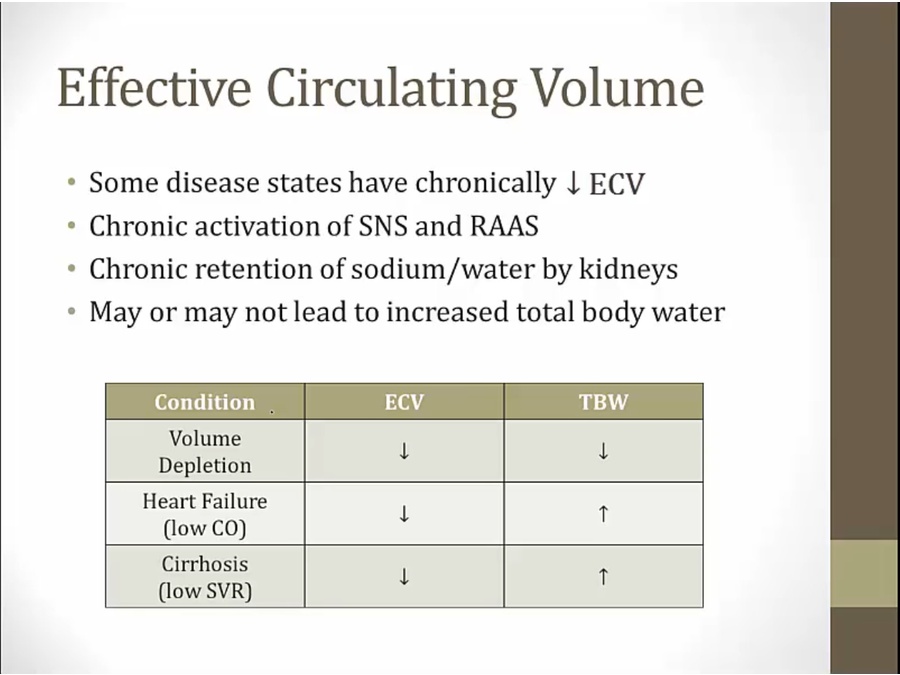
- cirrhosis: low SVR due to vasodilation
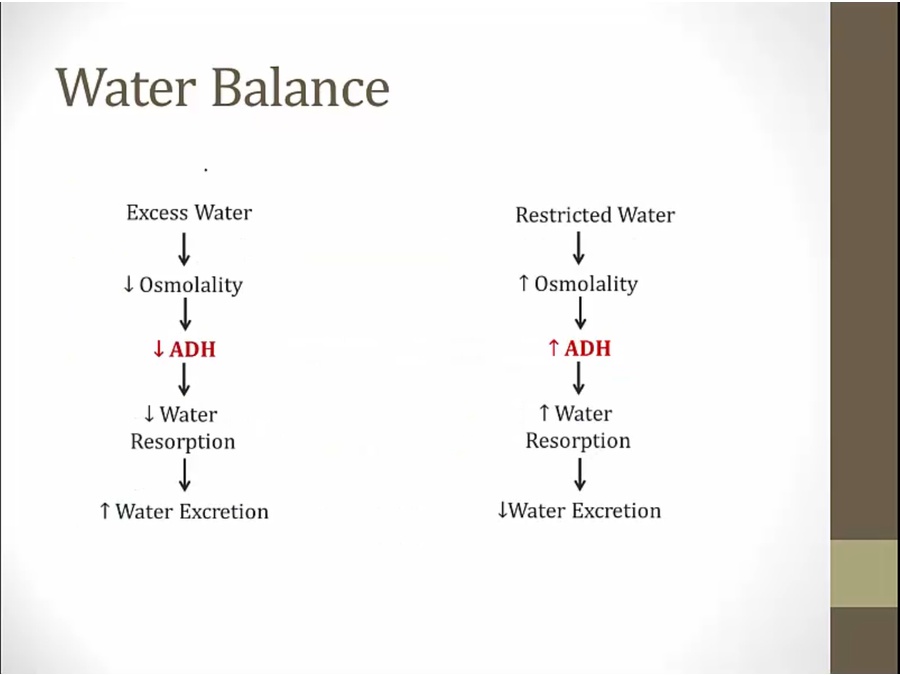
ADH
- only at very low level
- when activated at low ECV, can increase water reabsorption too much = hyponatremia
Water Balance
- any water intake must be excreted to balance normal Na
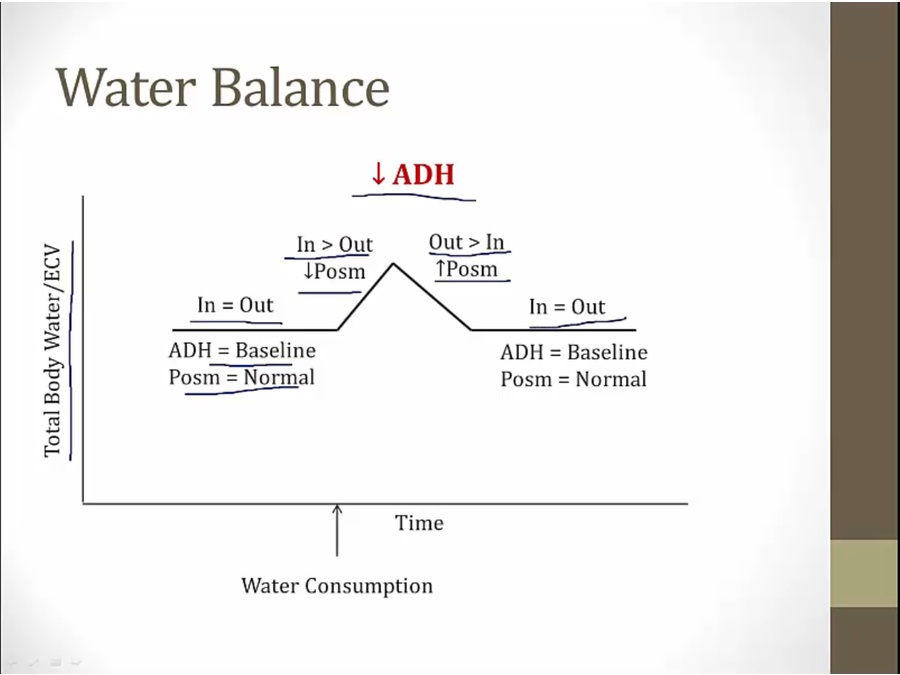
- starting point same level as stopping point
Na Balance
- water intake by itself only transiently increase ECV. Very quickly restored by decrease ADH
- Na intake increase ECV but not restored to normal level
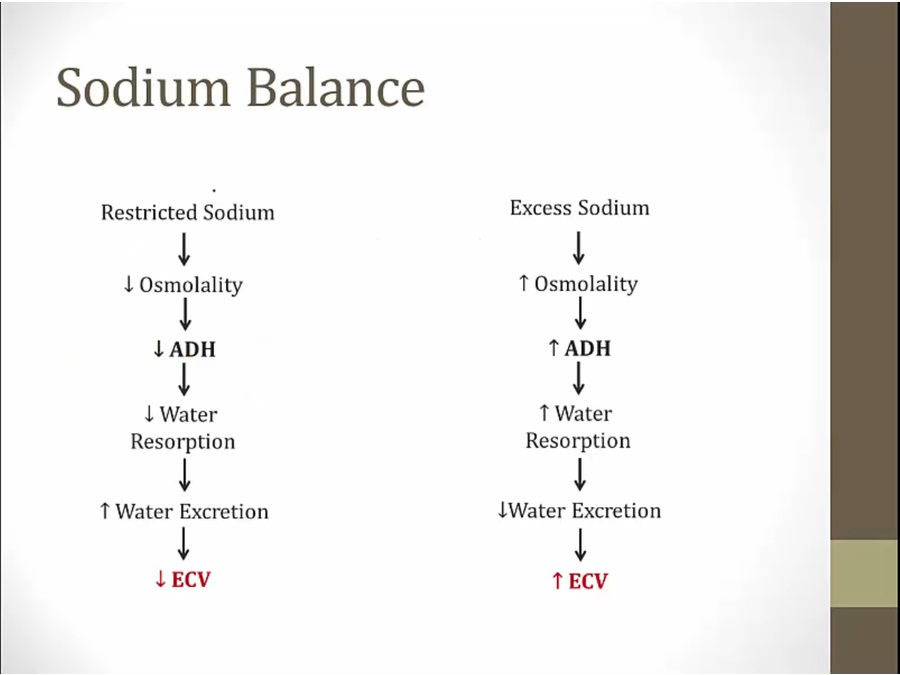
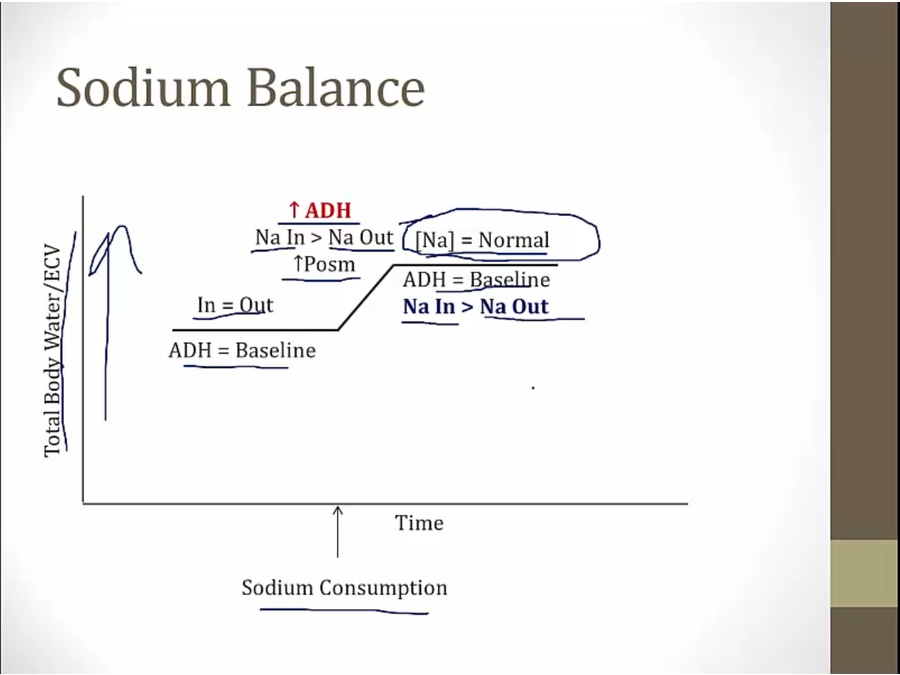
- abnormal high Na ingestion > increase osm > increase ADH
- osmolarity fixed, but ECV goes up
- fix Na concentration but not Na balance
- how to fix? RAAS, sympathetic
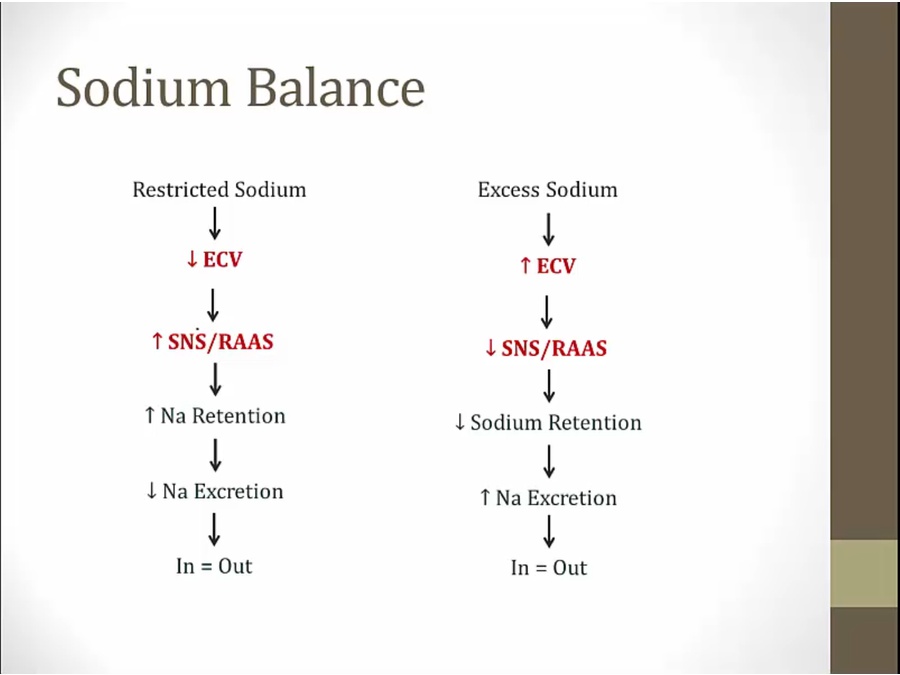
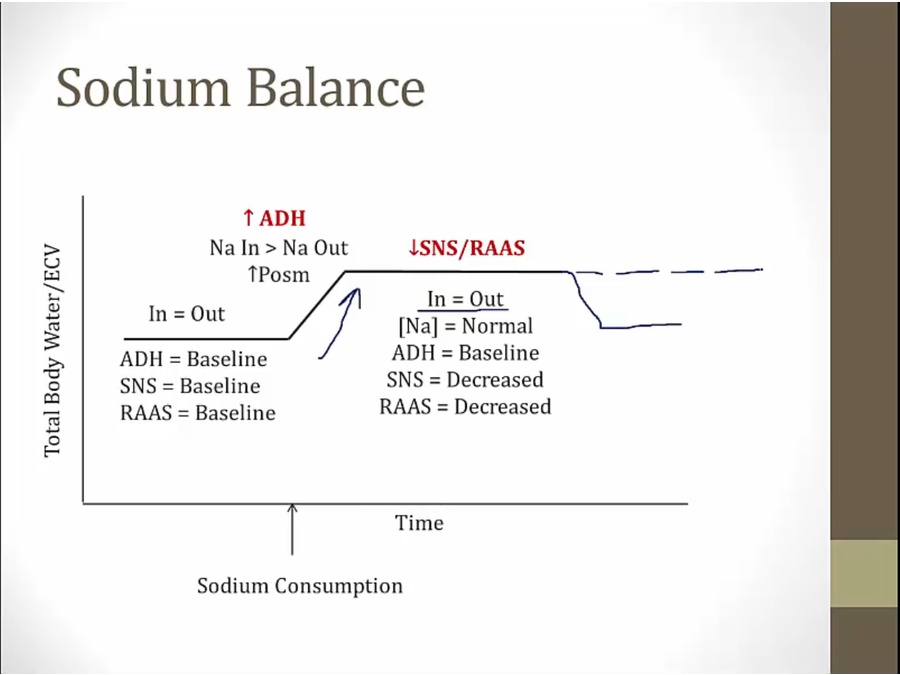
- decreased SNS/RAAS balances in vs out for Na/H2O but does not drive down ECV volume to original, only maintains it to have balanced Na/water
- body continue on higher ECV as long as Na consumption high
- only thing return to low ECV: lower Na consumption
- significance: HTN pts have high ECV volume (hypervolemia) despite Na/water balanced
- hypo/hypernatremia: problem of water balance, not Na balance
Pathology
- GI loss of Na and water
- very easy to have hyper/hyponatremia
- result: hypovolemic, hyponatremic
- Na excretion always reduced
- if eat a lot of Na, intake more than excretion
- often drink more free water than needed
- result: HF pts hypervolemic and hyponatremic
- result: SIADH pts euvolemic, hyponatremic
Links to this note