17 Nephritic Syndrome
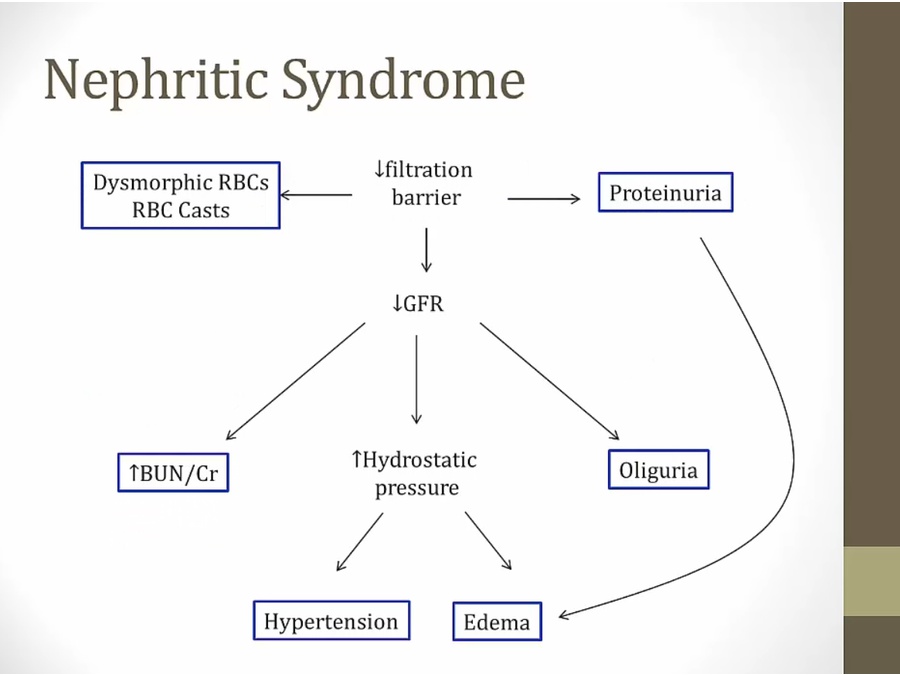
- increased hydrostatic pressure in rest of body
- GFR low: The glomeruli are stuffed full of cells, and blood flow slows way down.
Causes
- membranoproliferative: either nephritic or nephrotic
PSGN
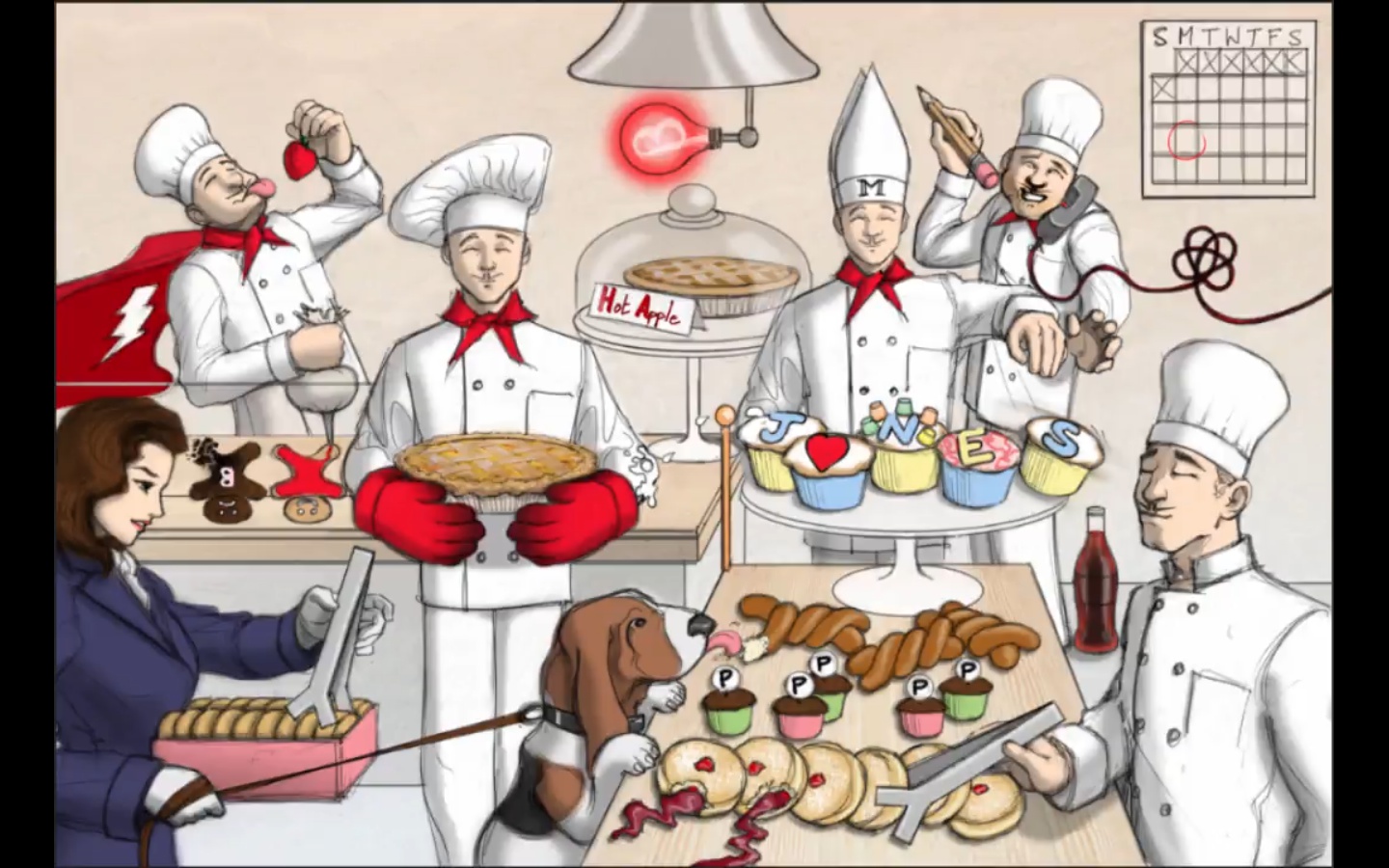
- rheumatic fever: master chef with M
- PSGN: post strep glomerulonephritis: chef on phone
- Facial puffs: Facial swelling seen in PSGN
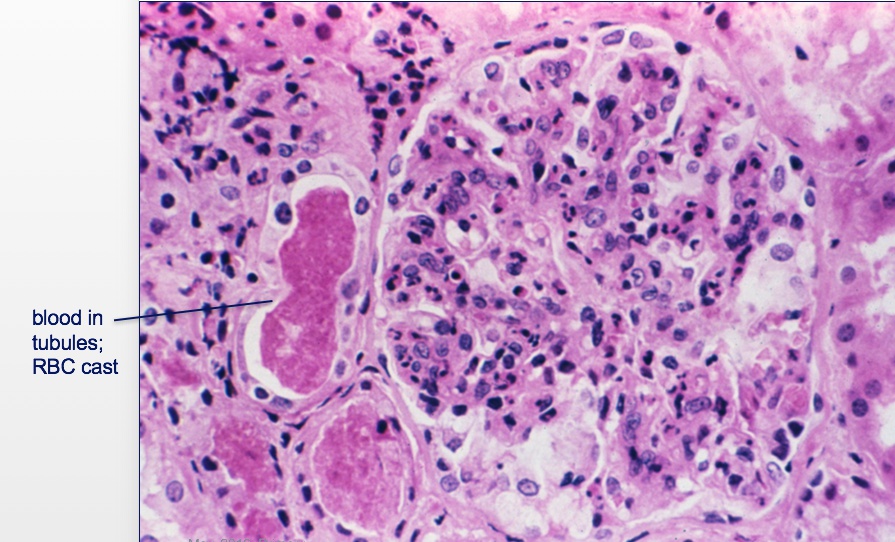
- Cola: Cola colored urine with PSGN
- Calendar: PSGN occurs 2 weeks after Strep infection
- Pencil: Early penicillin for treatment (prevents RF but not PSGN). Even though chef has pencil, he still has symptoms
- takes time for immune system
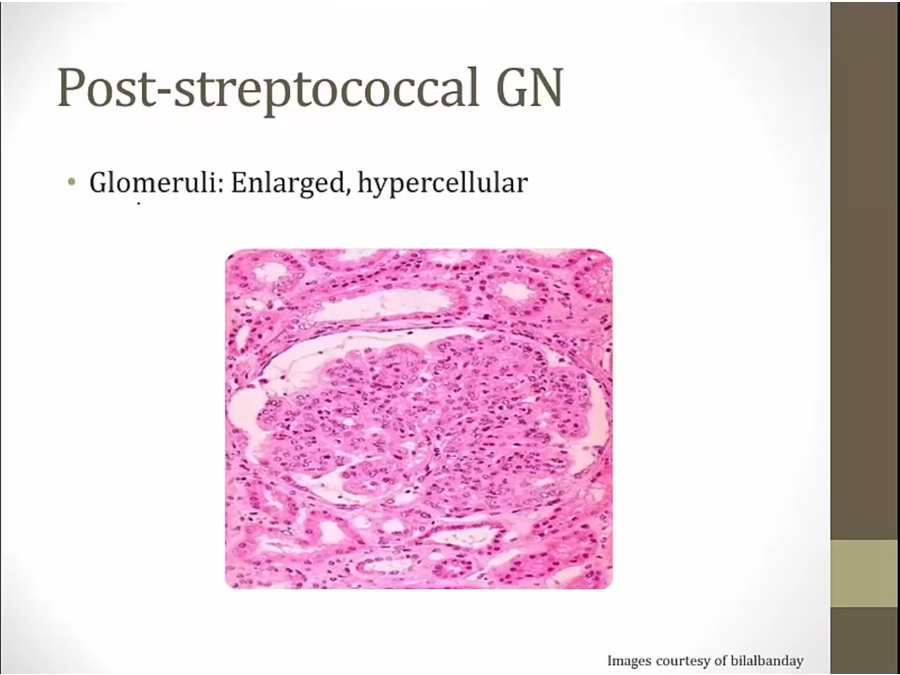
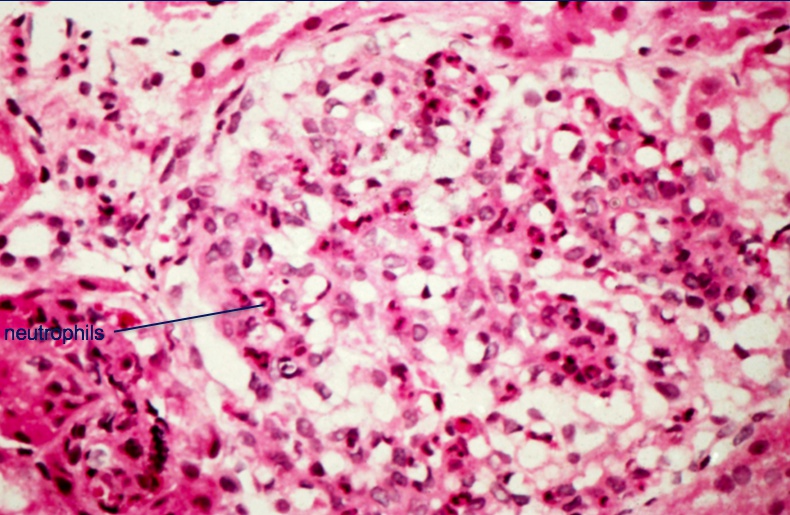
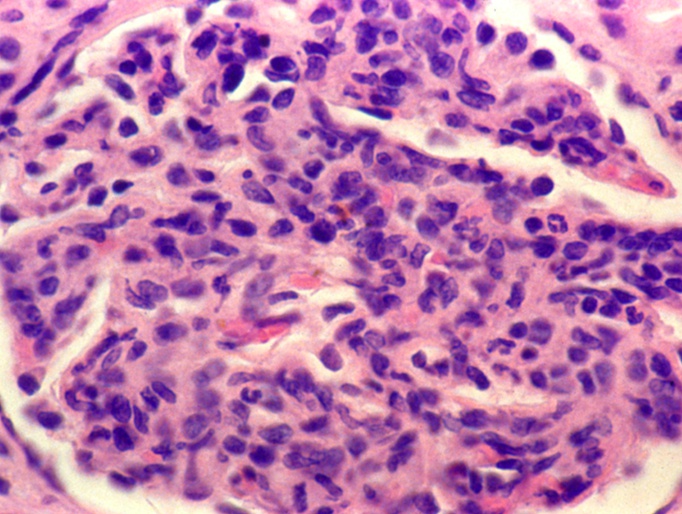
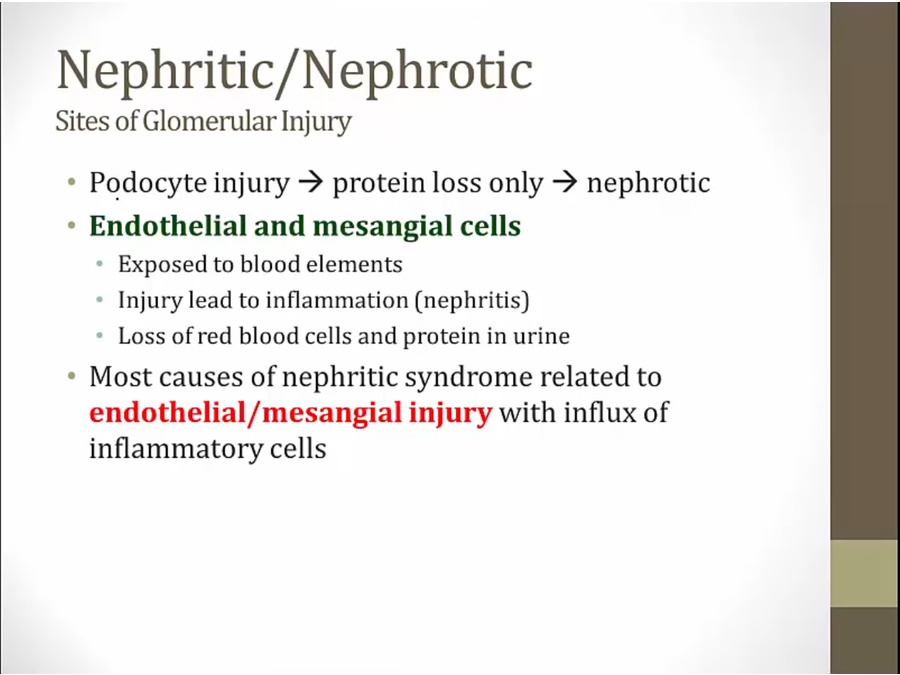
- hypercellular: inflammation related
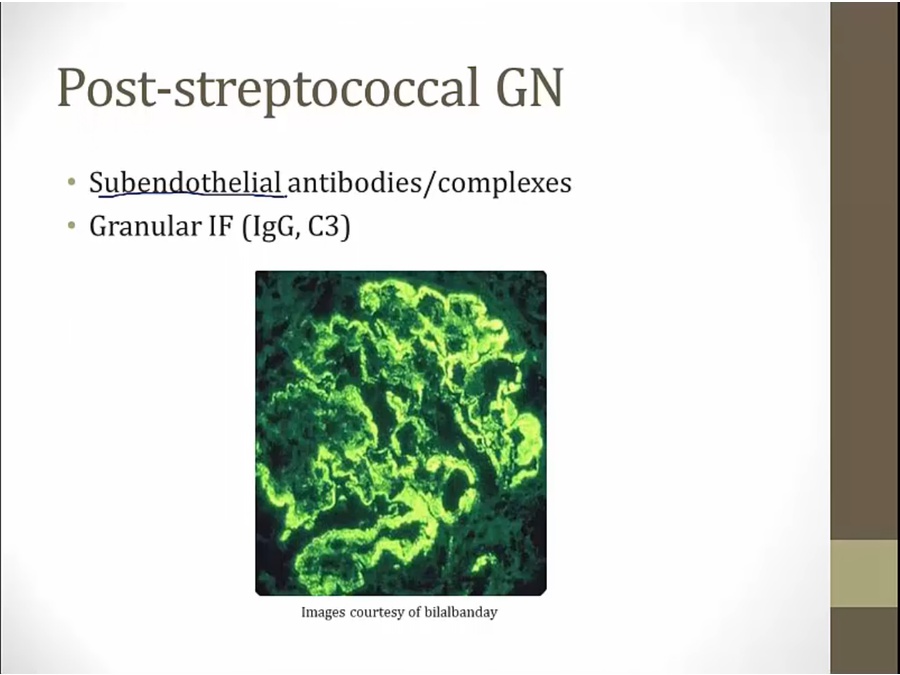
- bumpy appearance because in endothelium
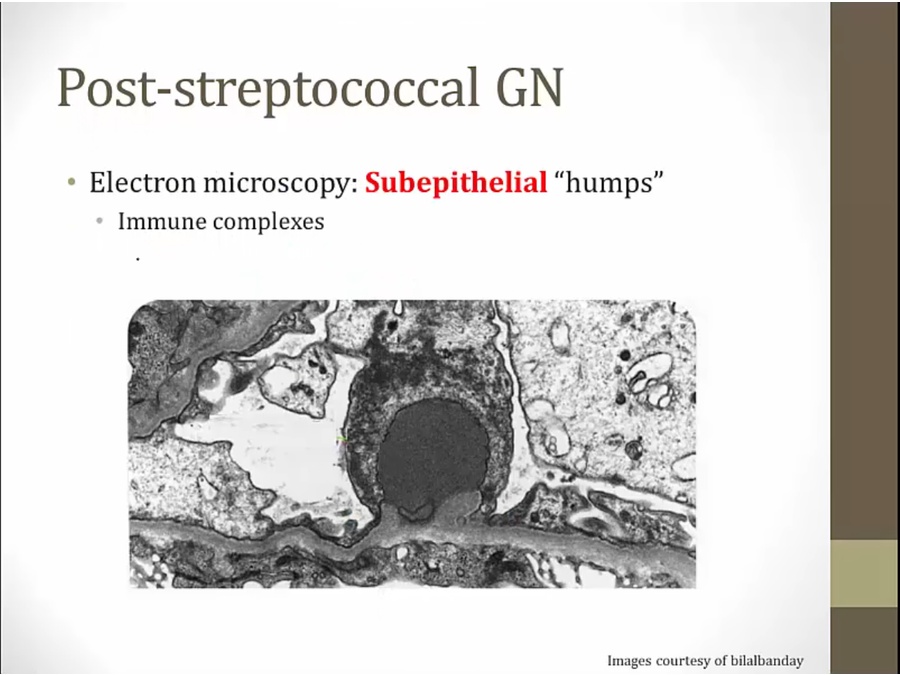
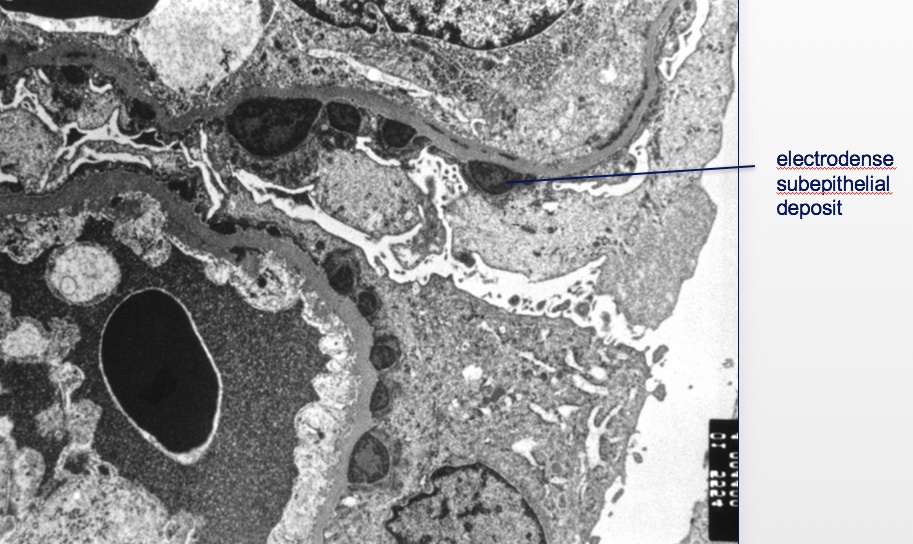
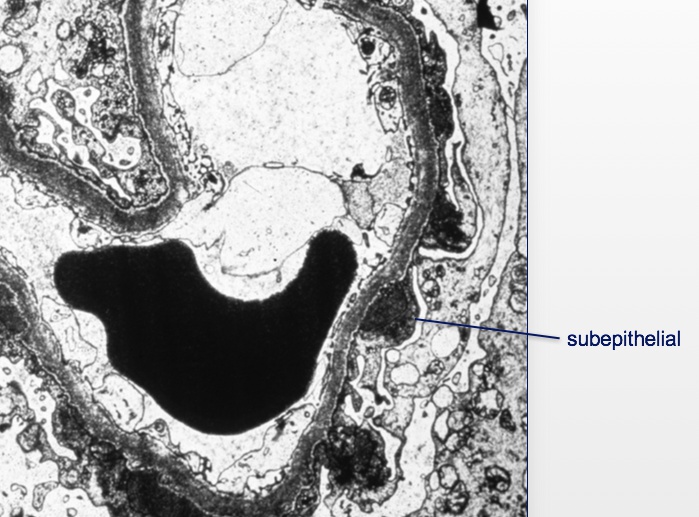
- worked their way into sub epithelium
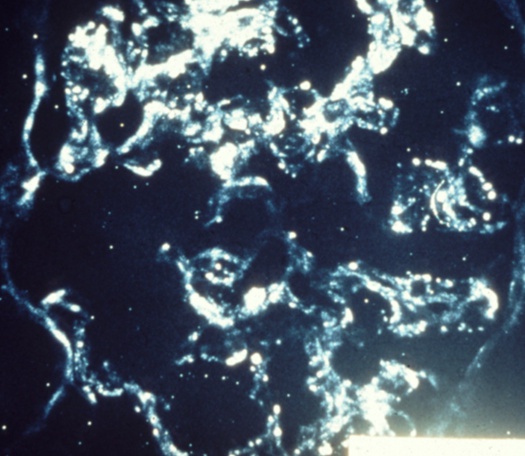
IgA
- IgA usually does not activate complement but does here
- weak complement activation, thus no hypocomplementemia
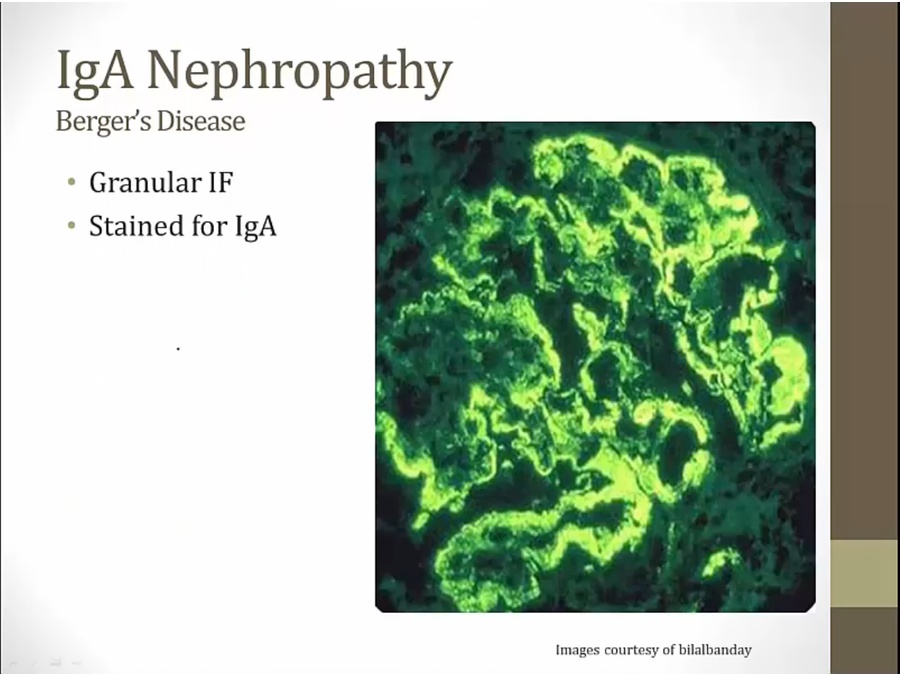
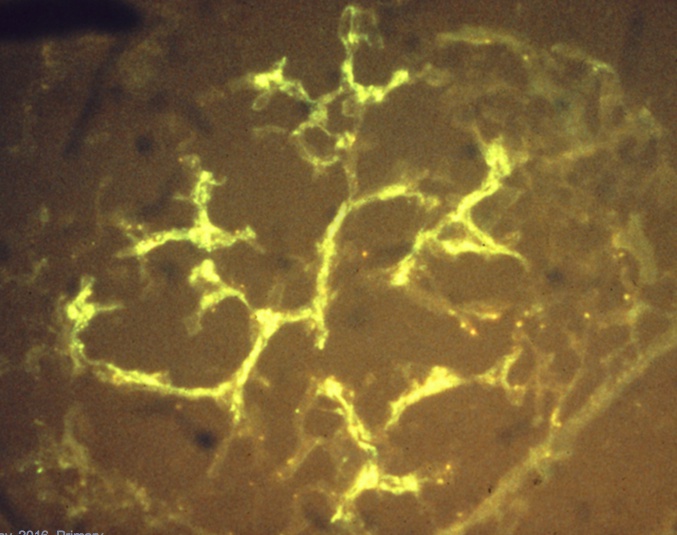
- IgA stain, like branches of tree
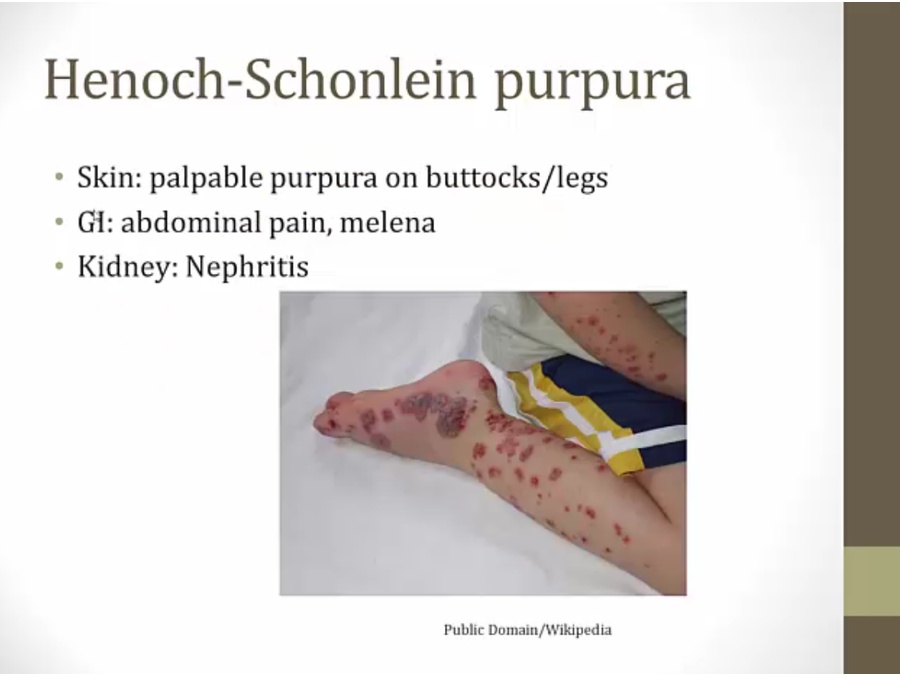
HS Purpura
- IgA deposition in joints, GI
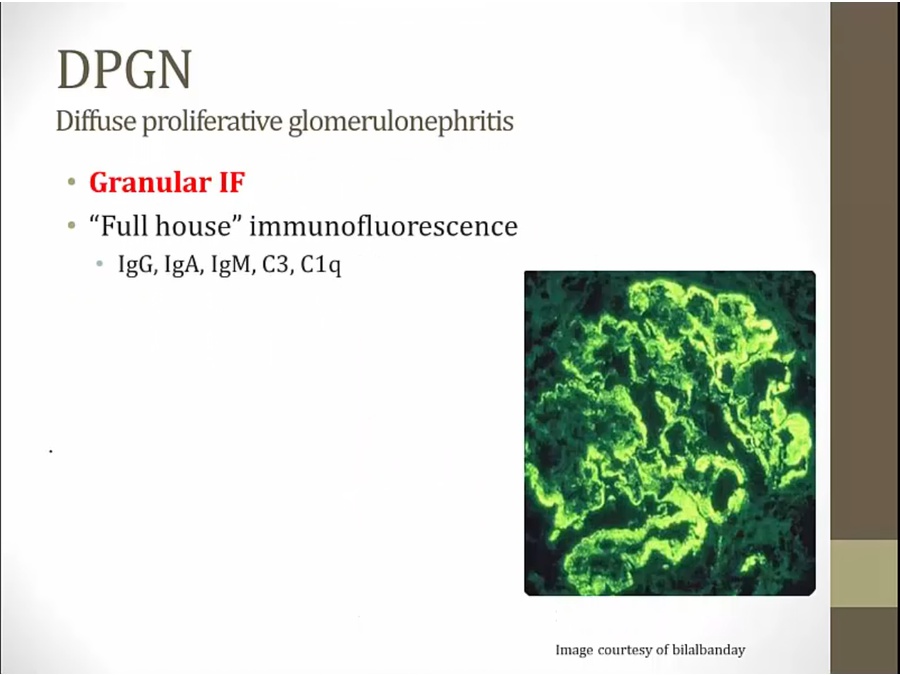
- IF stain granular
- complement activated via alternative/lectin pathway. IgA does not fix complement
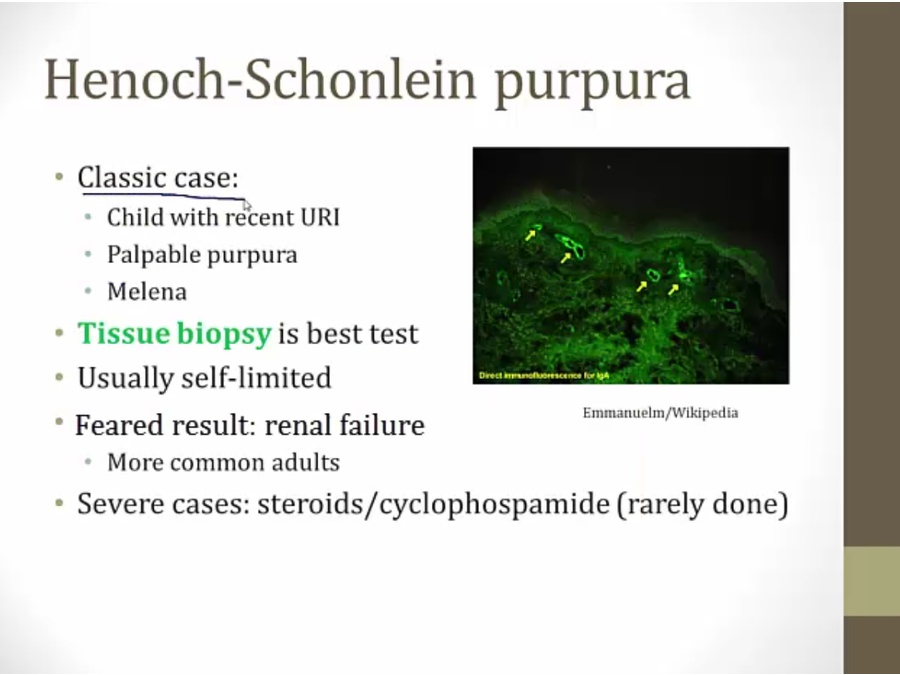
- biopsy shows IgA deposition
DPGN
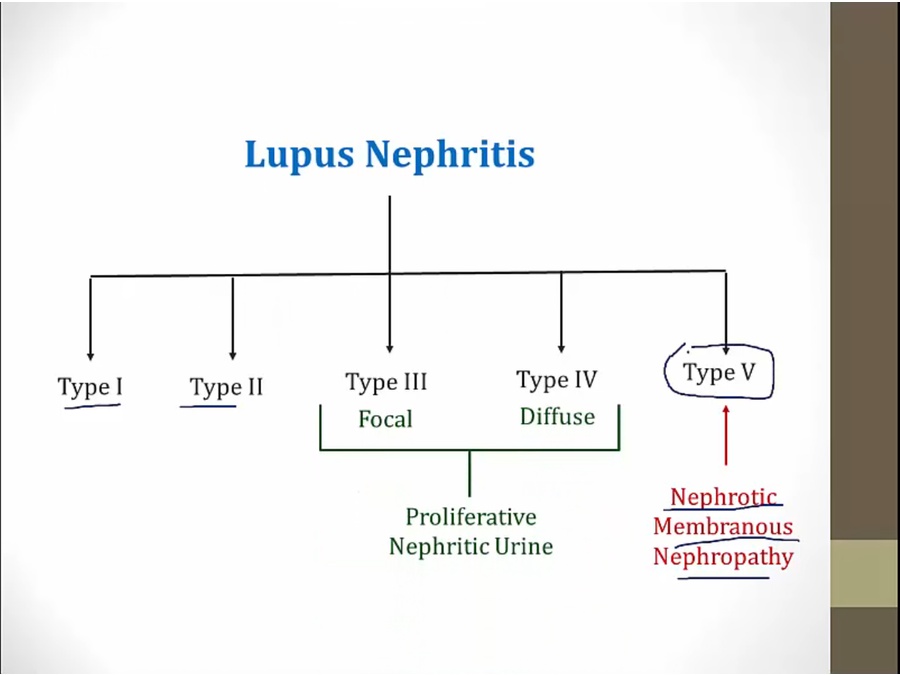
- type 1/2: mild; 3-5 serious
- focal: <50% glomerulus involved
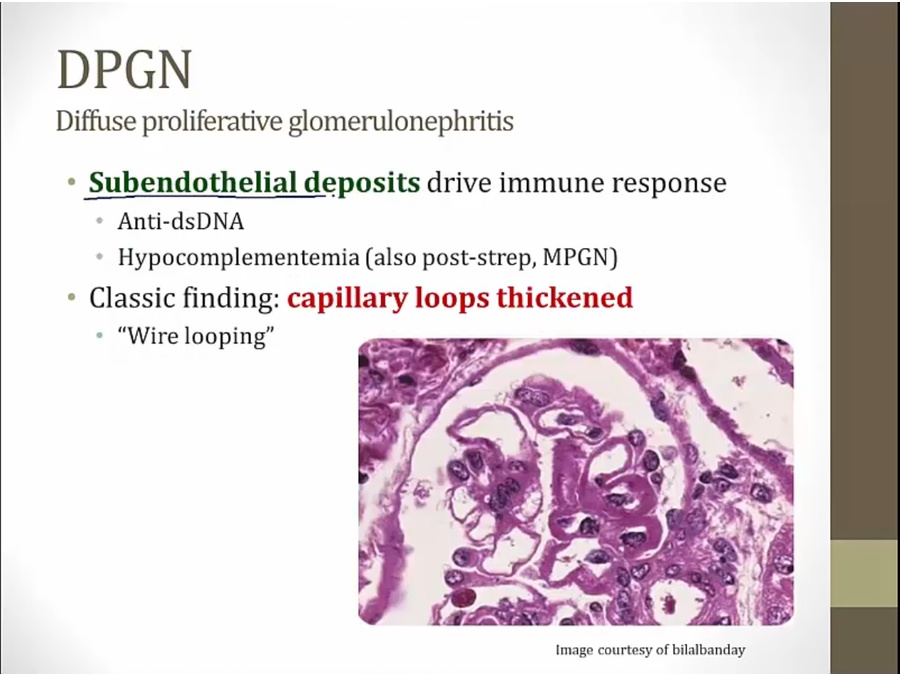
- immune response from anti-dsDNA
- can be nephrotic, nephritic
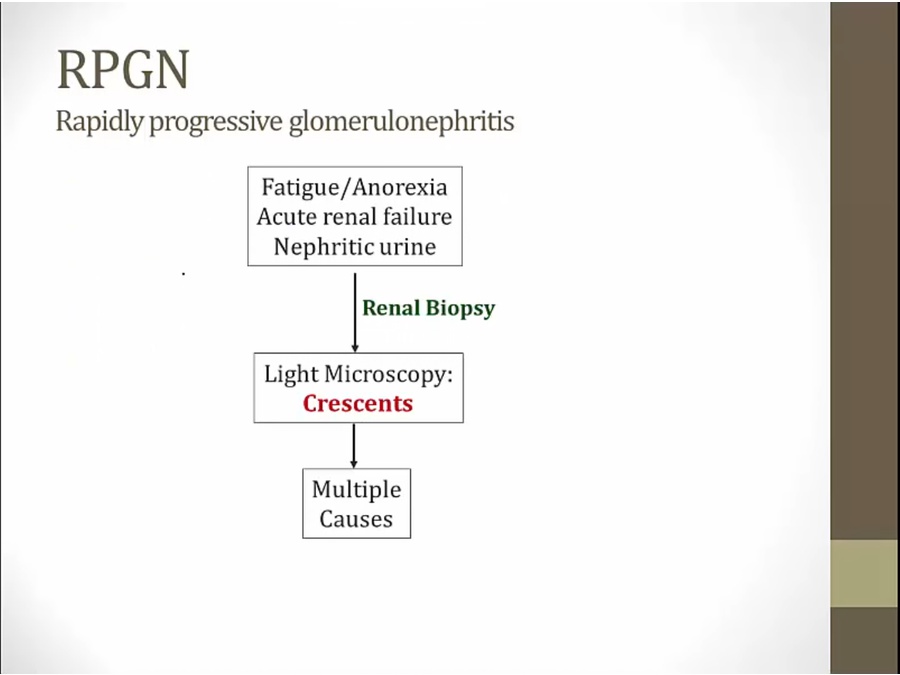
RPGN
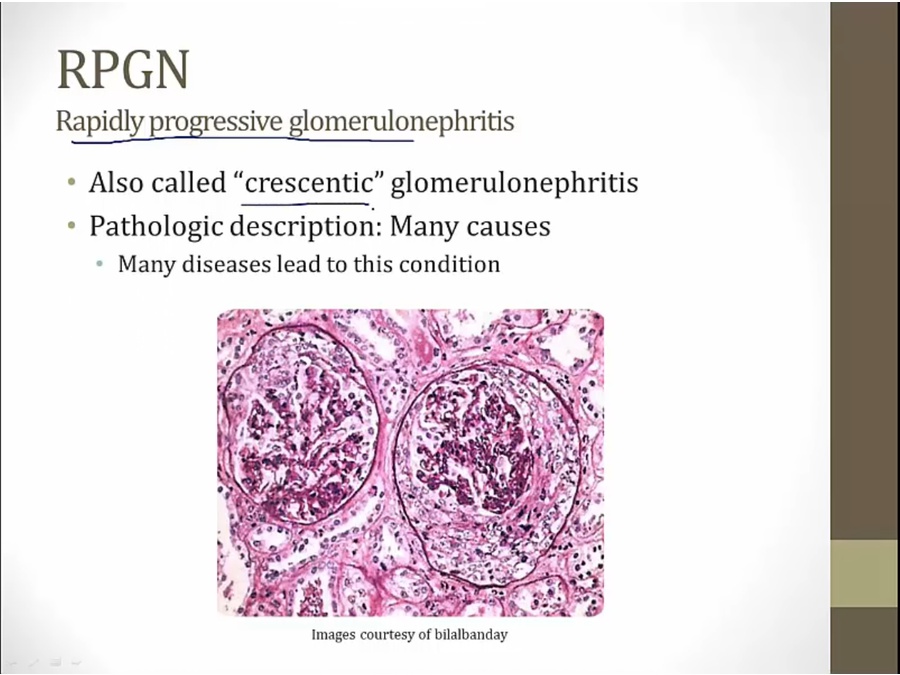
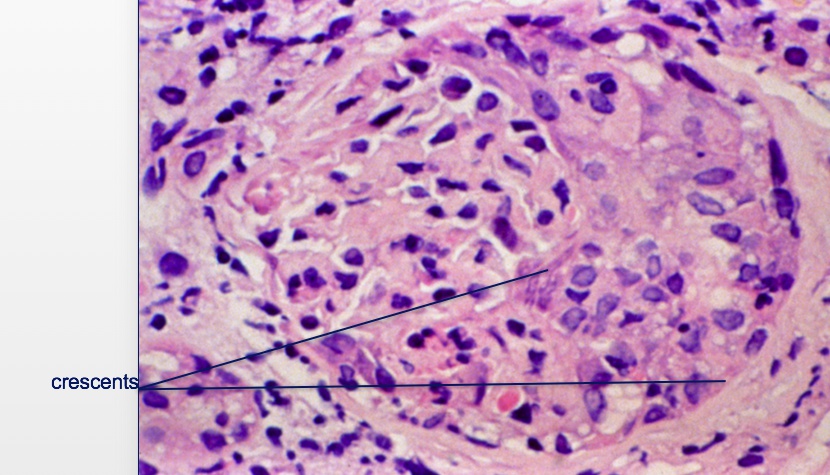
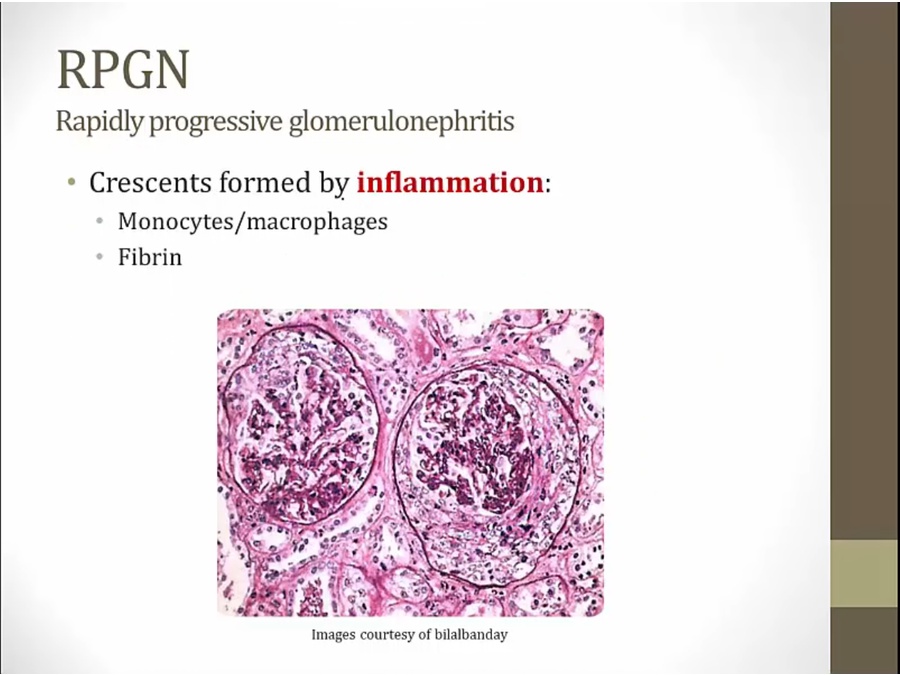
- RPGN: common pattern of inflammation in glomeruli representing many diseases
- quickly progress to RF
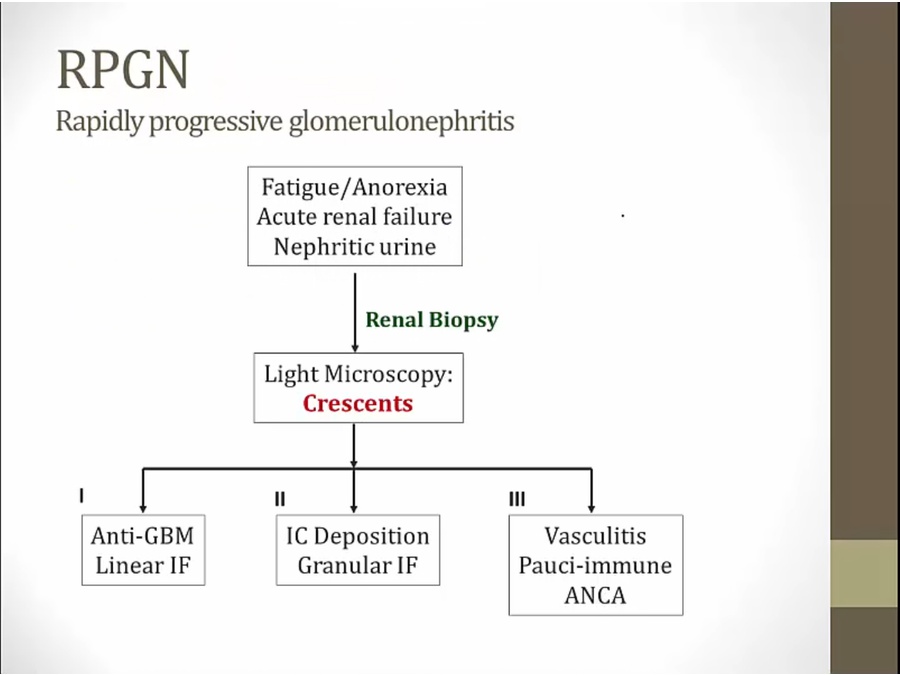
RPGN Type I
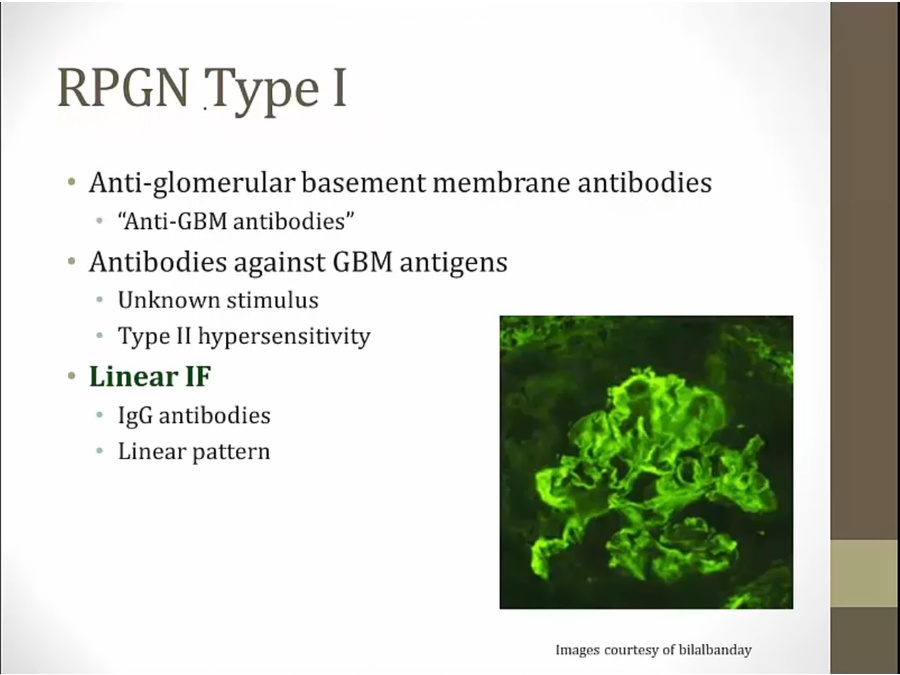
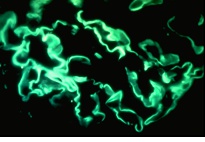
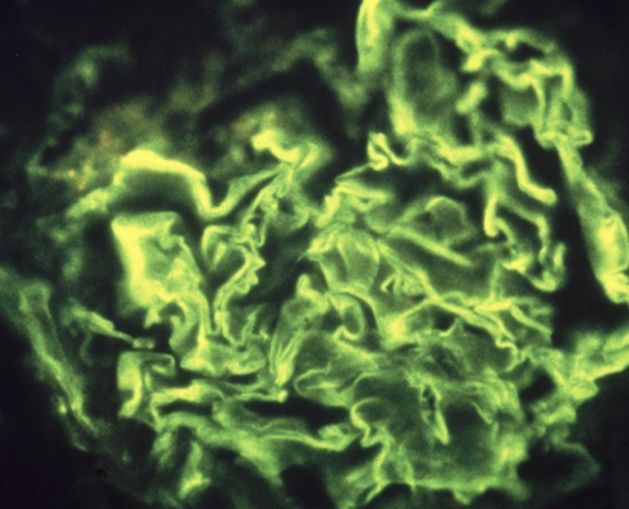
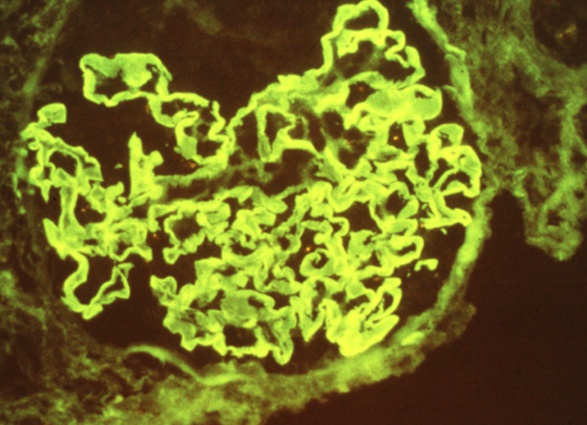
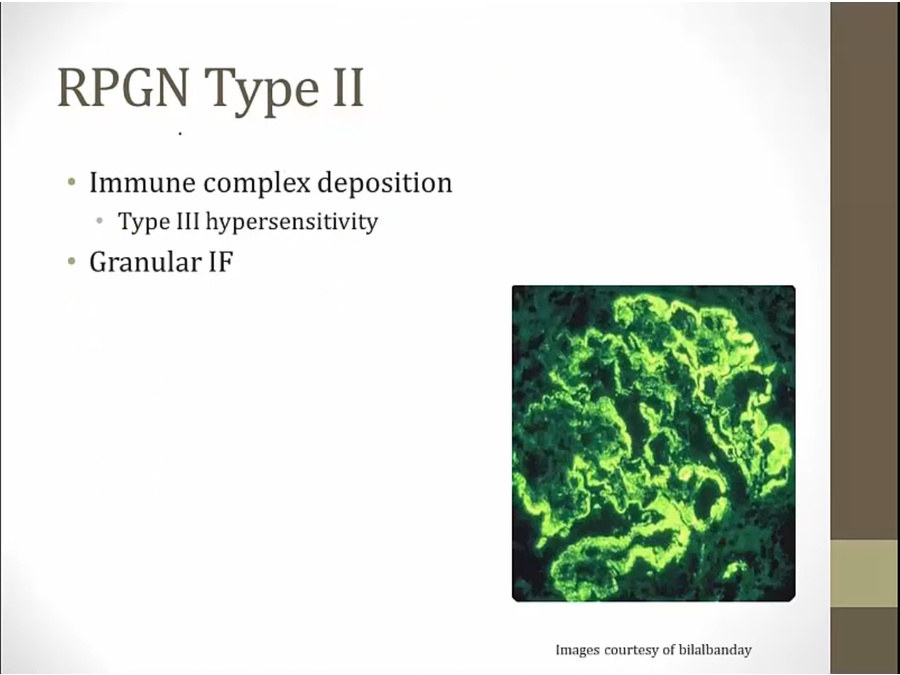
RPGN Type II
RPGN type III
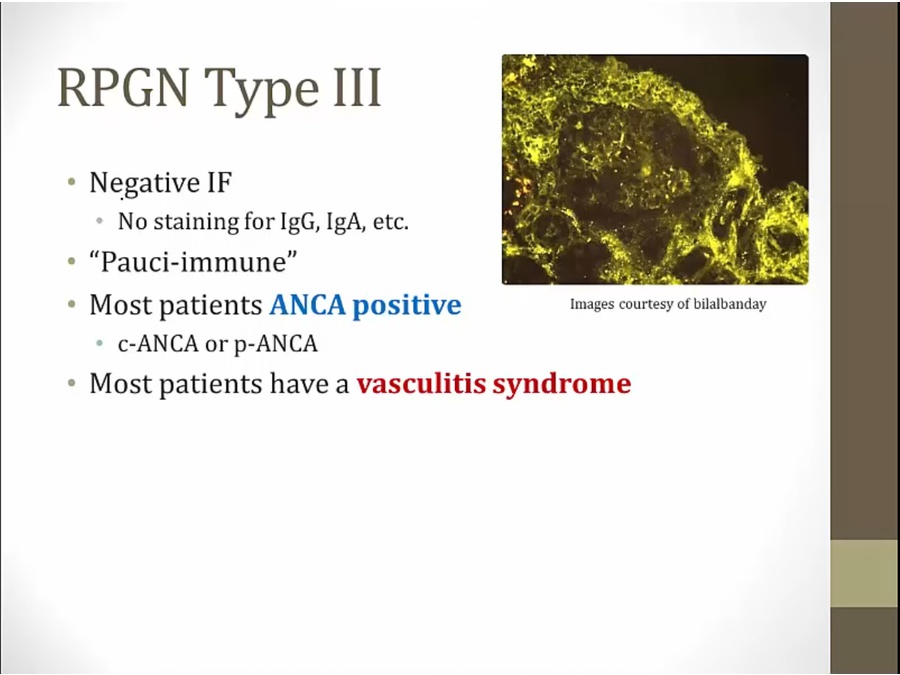
- Pauci-immune: no immune staining
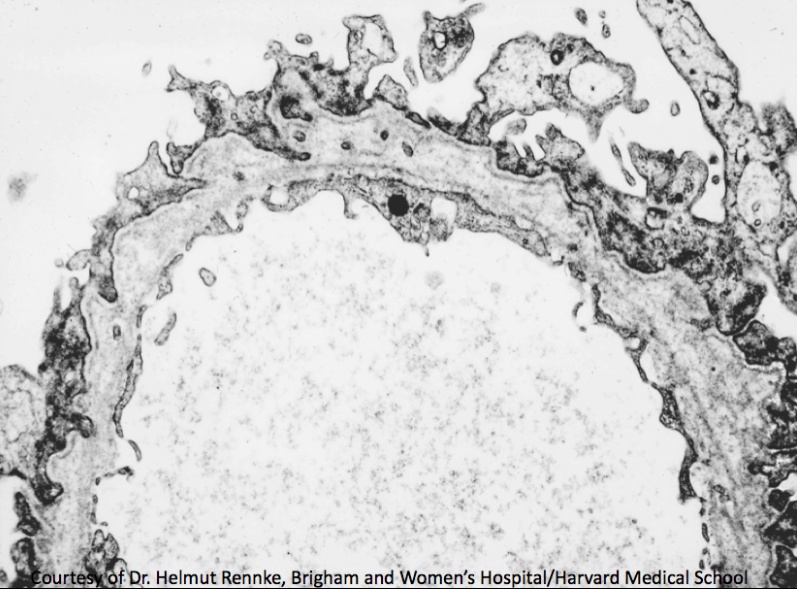
Alport
- male child with triad
- Electron microscopy of a renal biopsy shows irregular thinning of the glomerular basement membrane (GBM) with splitting/lamination of the lamina densa, giving the GBM a unique “basketweave” appearance.
Links to this note