acute diarrhea
- pathogenesis:
- mostly viral
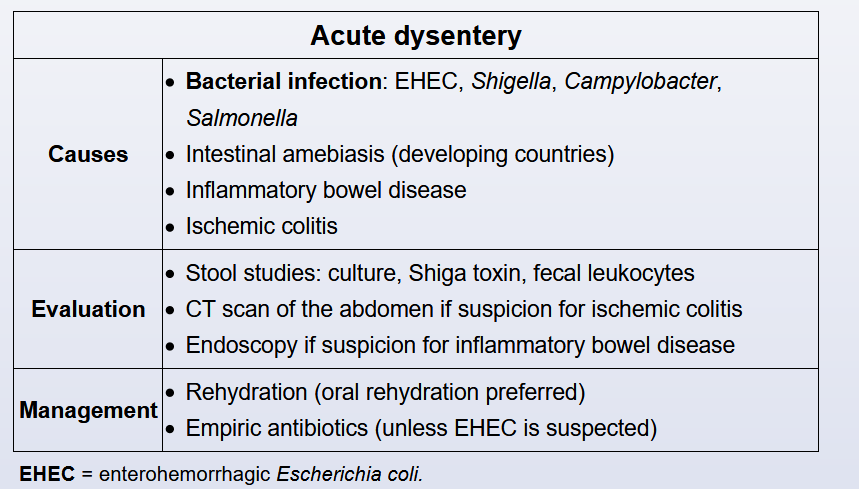
- if dysentery (with blood/mucus), then more likely bacterial
- bacterial: EHEC, Shigella, Campylobacter, Salmonella
- Noninfectious: IBD, ischemic colitis
- symptoms:
- last < 14 days
- watery diarrhea
- bacterial: more abdominal pain and systemic sx
- diagnosis:
- stool culture
- immunoassay for Shiga toxin
- fecal leukocyte count. An unexpectedly low fecal leukocyte count can suggest invasive amebiasis, although this is uncommon in developed countries.
- Imaging (eg, CT scan of the abdomen) is not usually needed unless there is suspicion for ischemic colitis. Endoscopy is not needed immediately for most patients but could be considered for those with recurrent or persistent (>2 weeks) symptoms
- treatment:
- mostly self limited
- bland, watery diarrhea and a self-limited course.
- empiric antibiotic therapy for patients with acute dysentery unless EHEC is suspected (antibiotic therapy in EHEC has been associated with increased risk for hemolytic uremic syndrome). However, oral antibiotics (eg, ciprofloxacin) are preferred.
Links to this note