acute rheumatic fever
- related: Infectious Disease ID, antibiotic prophylaxis for secondary prevention of rheumatic fever
- tags: #id
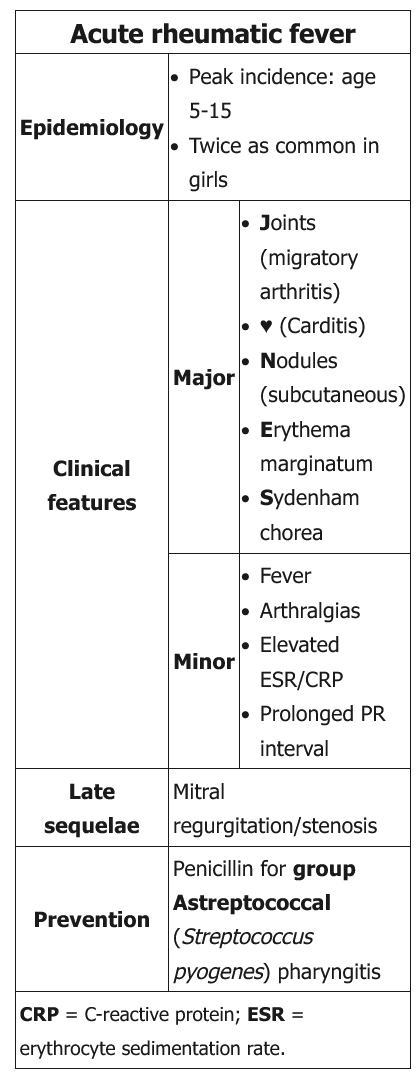
This patient’s history (recent emigration) and presentation with fever, arthralgias, migratory arthritis, subcutaneous nodules, mitral regurgitation murmur, and elevated erythrocyte sedimentation rate (ESR) are suggestive of acute rheumatic fever (ARF). Rheumatic fever occurs 2-4 weeks after pharyngeal infection with group A β-hemolytic Streptococcus (GAS).
ARF is a clinical diagnosis that is typically made using the Jones criteria (Table). Evaluation includes assessment of cardiac function and acute phase reactants (ESR and C-reactive protein) along with one of the following studies to establish GAS infection:
- Positive throat culture for GAS (negative in 75% of patients with ARF)
- Positive rapid streptococcal antigen test
- Elevated or rising antistreptolysin O (ASO) antibody titer
Diagnosis of ARF is based on evidence of GAS infection and 2 major (or 1 major and 2 minor) manifestations of the Jones criteria.
Patients must be treated with a full course of antibiotics to eradicate GAS carriage regardless of the presence of pharyngitis at the time of diagnosis. They are also at high risk for recurrence and progression of rheumatic heart disease with repeated episodes of GAS pharyngitis. Therefore, these patients must be treated with continuous antibiotic prophylaxis to prevent recurrent pharyngitis and limit progression of rheumatic heart disease.