alcoholic hepatitis
Symptoms
- fever, jaundice, tender hepatomegaly, leukocytosis
Diagnosis
- Labs: mildly elevated AST:ALT ratio > 2, high GGT, high INR, thrombocytopenia, elevated MCV
- clinical diagnosis: evidence of porrtal HTN with hx of consistent alcohol intake
- US or CT: steatosis, cirrhosis, portal hypertension
- Severity determined by Maddrey score: MDF score = 4.6 (prothrombin time – control prothrombin time) + total bilirubin (mg/dL)
- Can also use MELD score > 20 = moderate/severe disease
- Score of 32 or greater or hepatic encephalopathy defined as severe cases
Treatment
- Nonsevere, MDF < 32: supportive, no prednisolone
- thiamine, alcohol treatment
- Pentoxifylline not effective, do not use
- Severe: prednisolone (STOPAH trial showing improved 28 day mortality)
- CI includes active infection, UGIB, AKI, HCV/HBV, multiorgan failure
- Assess response on day 7 with Lille score, discontinue if no response >0.45
- Lille score less than 0.45: continue prednisolone for 28 days
Progonosis
- Alcohol abstinence can result in significant stabilization of liver function and reversal of portal hypertension.
- Liver transplantation is reserved for appropriate candidates who are at low risk for alcohol relapse.
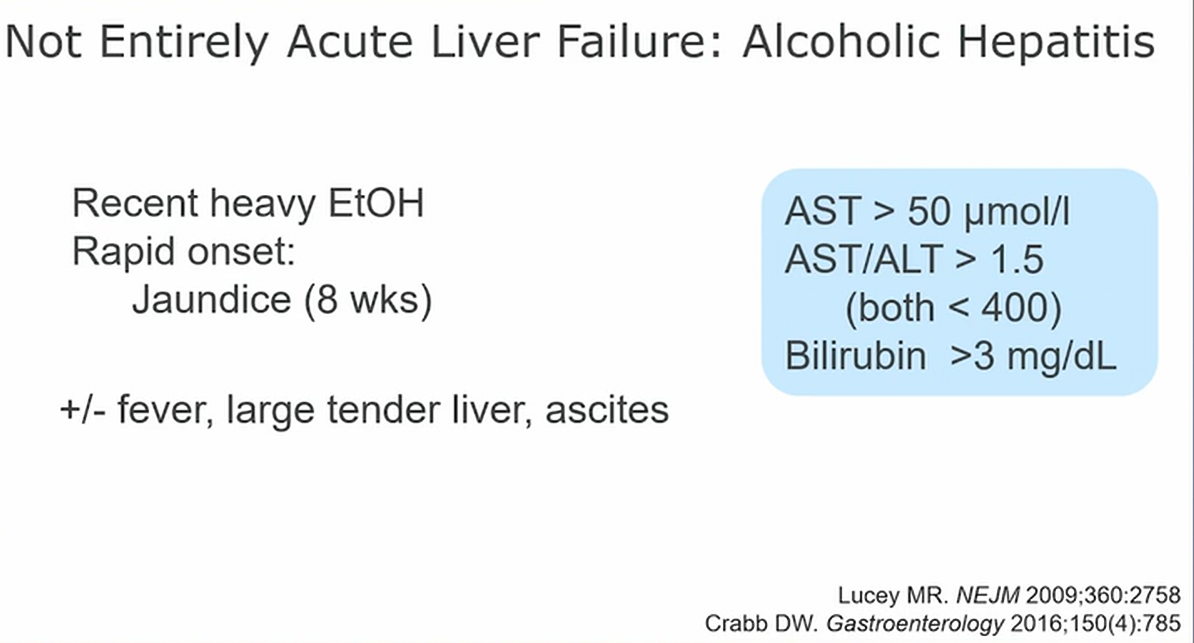
- not quite acute liver failure yet
- hx of alcohol use + more recent heavy alcohol
- may have ascites 2/2 underlying liver disease
- look for lab findings
- cholestatic picture. High bili, low transaminases
- rule out other causes of ALF: viral panel, anti smooth muscle, autoimmune hepatitis
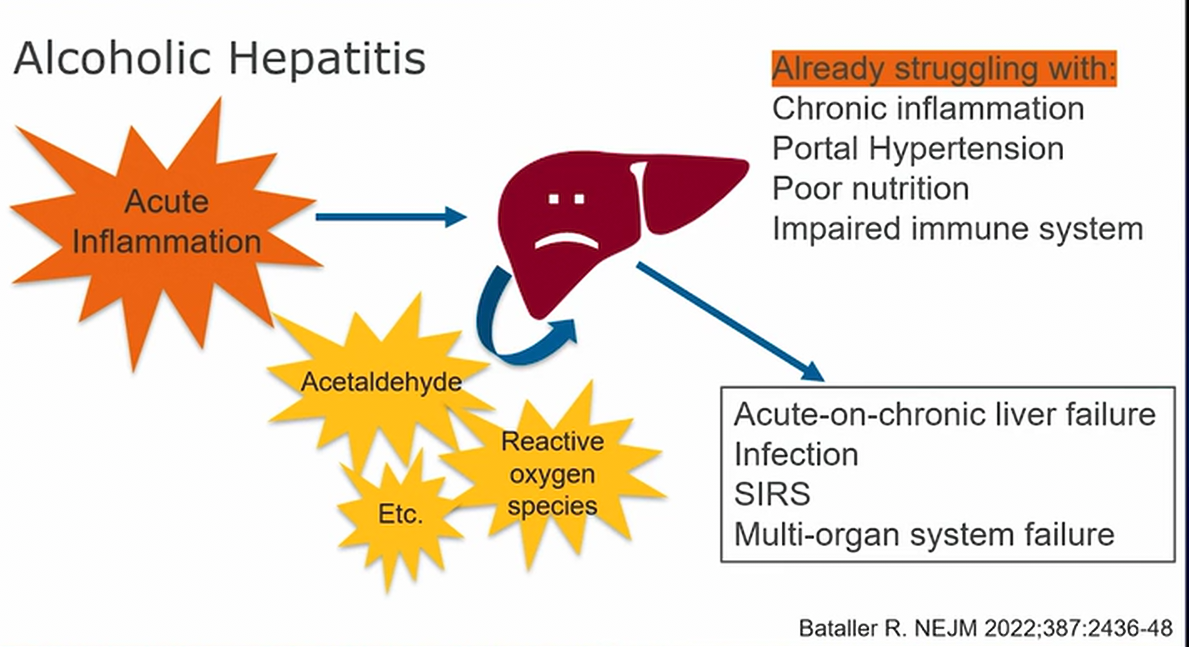
- chronic inflammation with portal hypertension, nutritional deplete
- acute inflammation on top can lead to acute liver failure
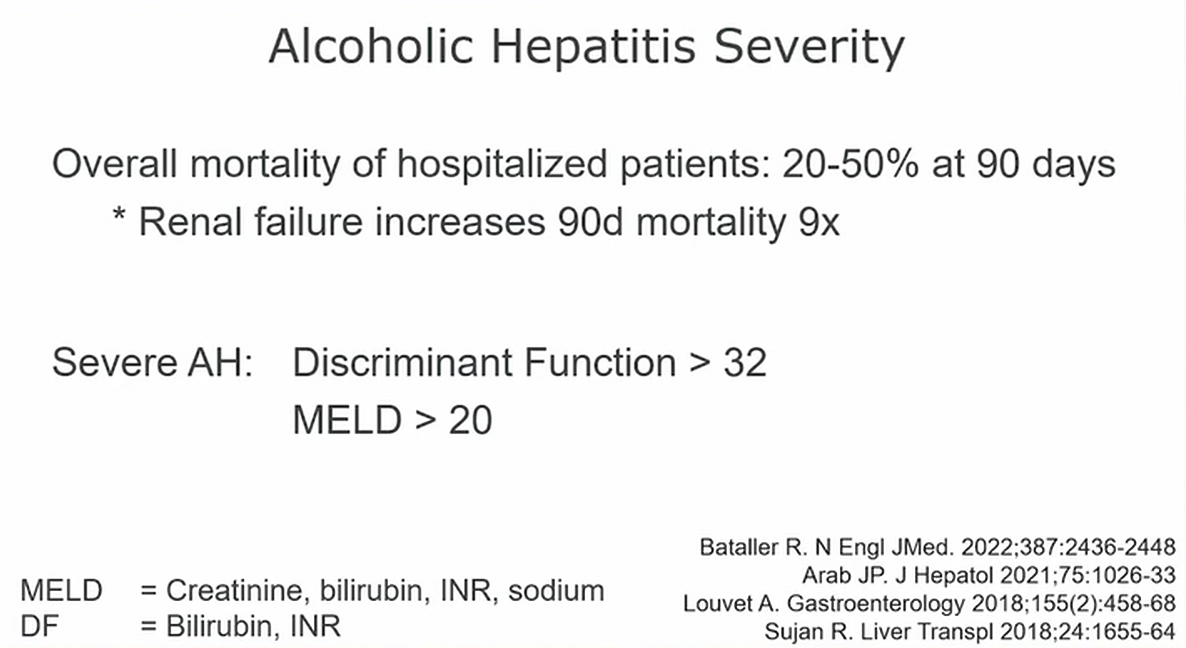
- use Maddrey’s discriminant function
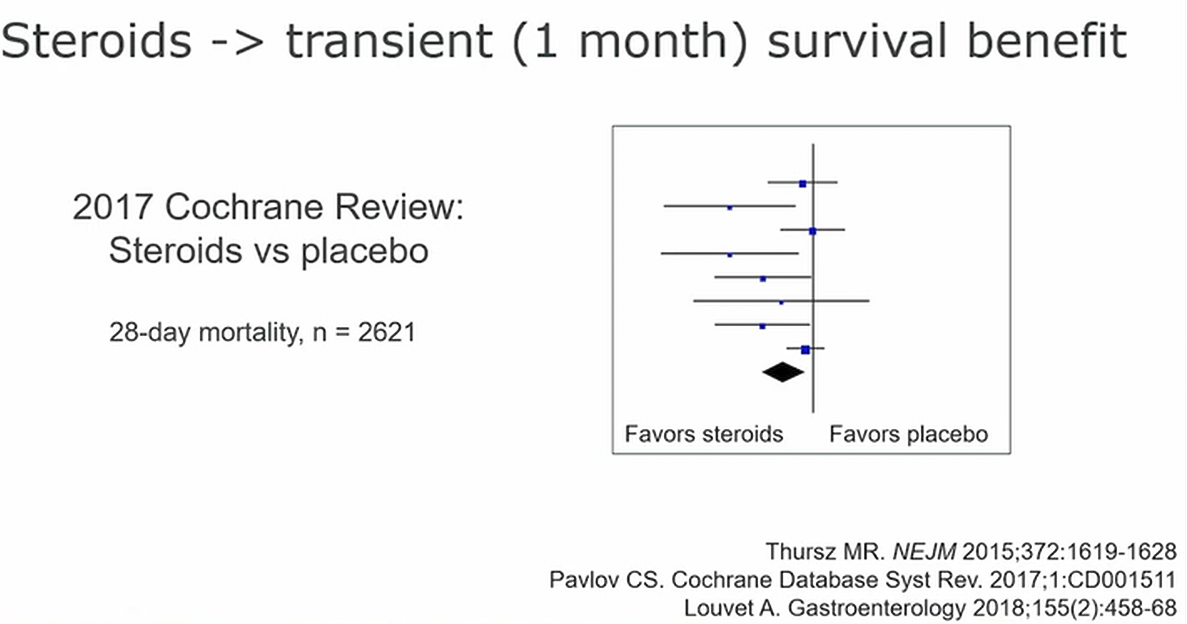
- after about a month, benefit disappears
- if not better in a week, stop steroids

- very clear data the No section is not helpful1
Links to this note