bowel regimens
Strategy
- Start with Miralax and senna-docusate once a day each
- Avoid lactulose if bowel is in colon as they will just sit there, absorb water, expand, and cause perforation
- Use manual disimpaction if bowel in rectum
- Can use dulcolax or lactulose suppository
- Use suppository next
- Use enema last
- Lactulose enema does not cause perforation
- Avoid electrolyte enema in renal patients: milk of magnesia, sodium phosphate
- Avoid anything rectal with leukemia patient
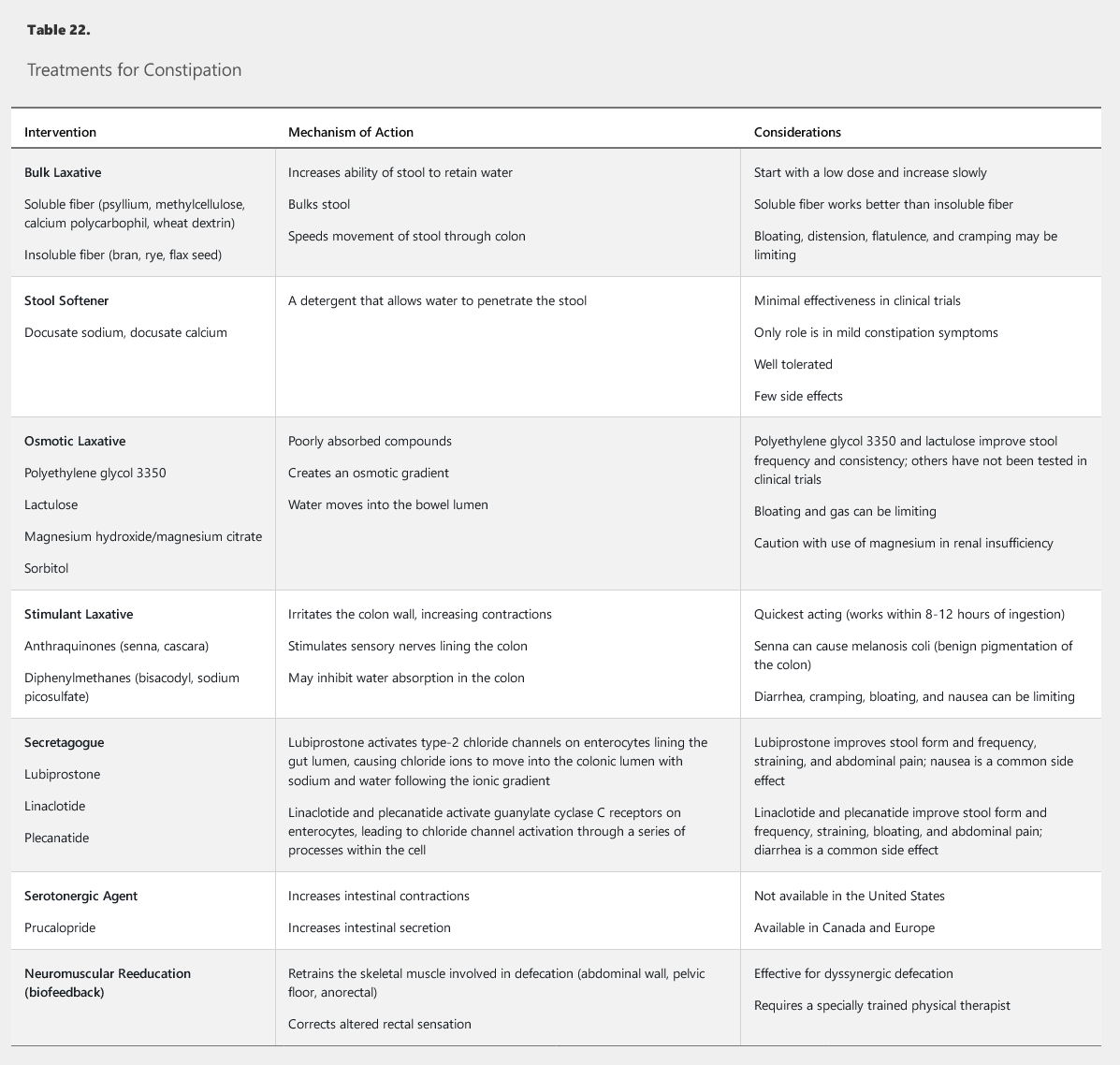
- mechanism: absorb water, increase stool mass
- side effects: gas, bloating
- fiber supplements
- Metamucil: psyllium seed
- Citrucel: methylcellulose
- Fibercon: calcium polycarbophil
- Benefiber: wheat dextrin
surfactants
- mechanism: lower surface tension of stool, allows water to enter
- cons: less effective
- Colace: docusate sodium
- docusate calcium
osmotic laxatives
- mechanism: causes intestinal water secretion
- side effects: bloating, volume overload, electrolyte disturbance
- Miralax/GoLytely: PEG, no need to use more than once a day
- Lactulose: synthetic disaccharide.
- Sorbitol: similar to lactulose
- Saline laxative: high magnesium, poorly absorbed, acts as hyperosmolar solution but use with caution for renal insufficiency patients
- milk of magnesia
- mag hydroxide
- glycerin/Glycerol
stimulants
- mechanism: increase contraction, stimulates sensory nerves, quickest acting, 8-12 hours
- SE: gastric irritation, melanosis coli with senna
- Dulcolax: bisacodyl
- Senokot: senna
disimpaction
suppository
- small pill injected in the rectum
- can liquidify stool and overcome obstruction
- glycerin
- Dulcolax: bisacodyl
enemas
- liquid injected in rectum
- soapsuds: soap with water
- tap water: good for older adults because safer than sodium phosphate enema
- saline enema
- milk & molasses
- mineral oil enema, used usually after disimpaction. Softens stool and provides lubrication
- sodium phosphate enema: associated with hypotension, hypoCa, hyperP, hypo/hyperK
secretagogue
- Lubiprostone: type 2 chloride channel activation, cause chloride to move into colon, ionic gradient
- Linaclotide/plecanatide: CGMP activation, chloride release
opioid antagonist
- naloxegol, oral naldemedine, SQ methylnaltrexone
Links to this note