cardiac arrest in pregnant patients
- related:
- tags:

To treat the critically ill pregnant patient:
- Place the patient in the left-lateral decubitus position to relieve possible compression of the inferior vena cava. Uterine obstruction of venous return can produce hypotension and could precipitate arrest in the critically ill patient.
- Two methods of supporting the patient in the left-lateral decubitus position are (1) to use the angled backs of 2 or 3 chairs or (2) to use the angled thighs of several providers. Overturn a 4-legged chair so that the top of the chair back touches the floor. Align 1 or 2 more overturned chairs on either side of the first so that all are tilted in the same manner. Place the woman on her left side and align her torso parallel with the chair backs. Remember that this position will not be practical if chest compressions are needed.
- Give 100% oxygen.
- Establish IV access above the diaphragm and give a fluid bolus.
- Assess for hypotension; maternal hypotension that warrants therapy is defined as a systolic blood pressure (SBP) less than 100 mm Hg or less than 80% of baseline. Maternal hypotension can cause a reduction in placental perfusion. In the patient who is not in arrest, both crystalloid and colloid solutions increase preload.
- Consider reversible causes of cardiac arrest and identify any preexisting medical conditions that may be complicating the resuscitation.
Shifting Gravid Uterus
In cardiac arrest, the reduced venous return and cardiac output caused by the gravid uterus puts the mother at a hemodynamic disadvantage, thereby potentially reducing the effective coronary and cerebral perfusion produced by standard chest compressions. Therefore, when there is aortocaval compression, the effectiveness of the chest compressions may be limited. Patient positioning has emerged as an important strategy to improve the quality of CPR and the resultant compression force and cardiac output.
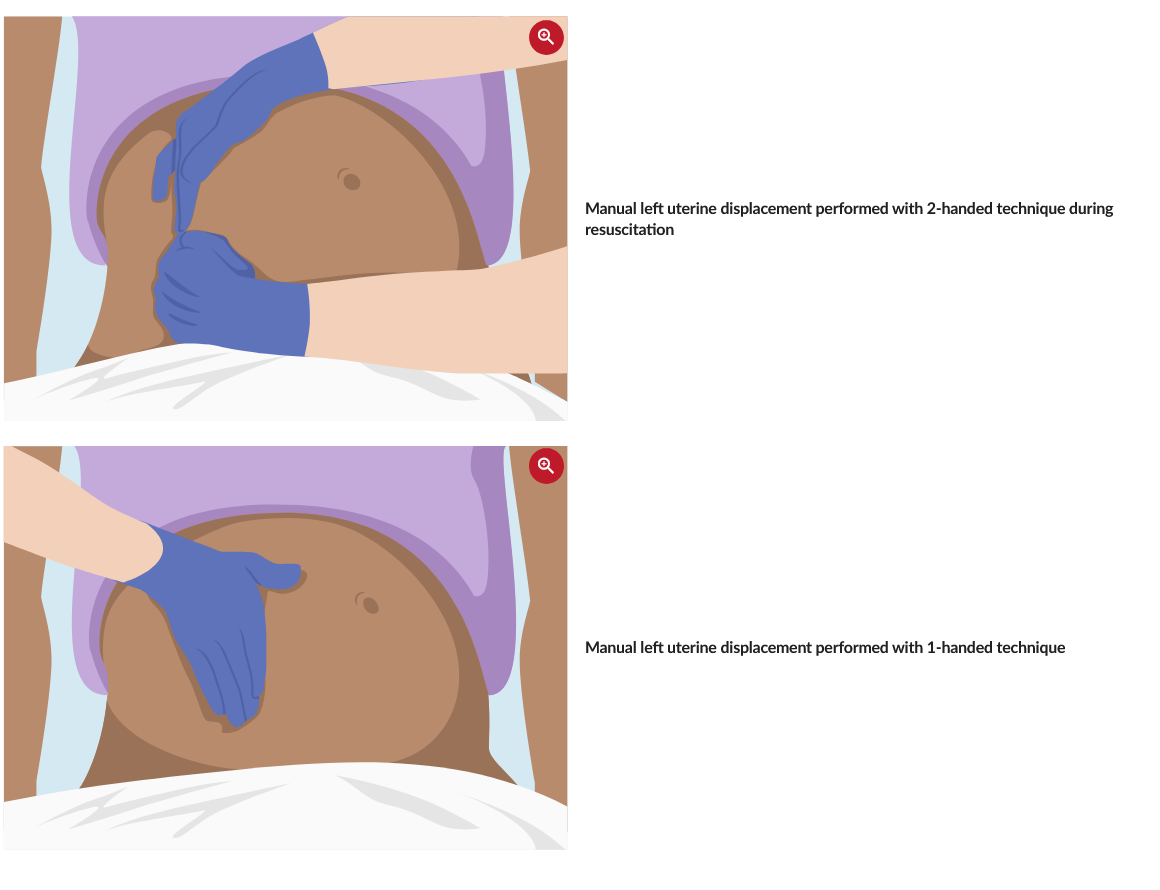
Relieve compression of the inferior vena cava and the aorta by shifting the gravid uterus left and upward off the matemal vessels:
- Stand on the left side of the patient, level with the top of the uterus.
- Reach across the midline with both hands and pull the gravid uterus leftward and upward toward your abdomen.
- If it is not possible to stand to the left of the patient, use one hand to push the gravid uterus to the patient’s left and upward.
Chest Compressions
Chest compressions performed while the patient is tilted are not ideal Although it is feasible to perform chest compressions in the tilted patient, chest compressions performed in the tilted position are less forceful when compared with the supine position. However, there are no physiologic data available for chest compressions in the tilted position. High-quality chest compressions are essential to maximize the chance of a successful resuscitation. An alternative method of relieving aortocaval compression, such as manual displacement, maybe more practical and ideal during resuscitation because it allows for continuous and easier delivery of all other aspects of resuscitation, including high-quality chest compressions, defibrillation, IV access, and intubation.