foreign body aspiration
- Keywords: Pediatric
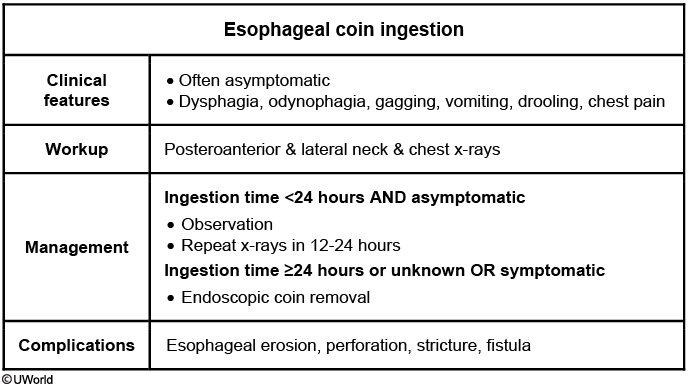
- Obtain 2-view (posteroanterior [PA] and lateral) neck and chest x-ray top confirm the location of the foreign body
- an esophageal coin appears linear on lateral x-ray; a tracheal coin appears linear (project on end) in the PA view.
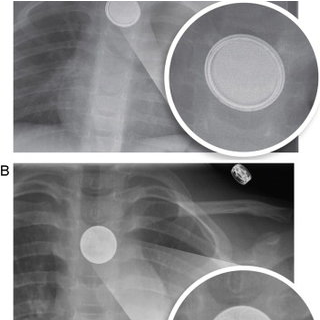
- Xray also distinguishes between a coin and battery (the latter can cause perforation in just a few hours).
- A coin is seen in this patient’s x-ray as a homogenous object with a sharp, crisp edge; the bilaminar structure of a button battery causes a “double-ring” sign.
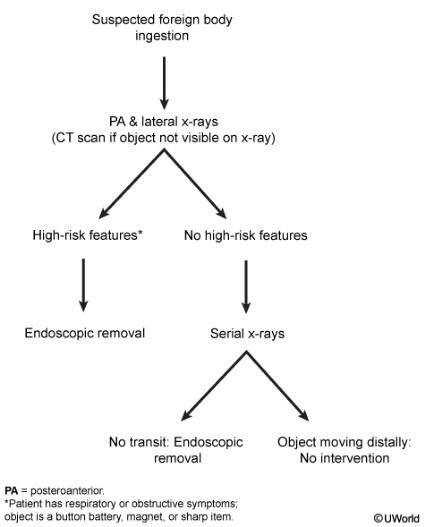
- Coins are the most common gastrointestinal foreign bodies. They are considered low risk due to the lack of sharp edges and nontoxic material. High-risk objects (eg, button batteries, magnets, sharp items) typically require endoscopic removal regardless of symptoms due to the risk of necrosis and perforation of the gastrointestinal tract.
- Asymptomatic patients with coin ingestion <24 hours earlier can be observed with repeat x-rays in 12-24 hours to ensure passage beyond the pylorus. Children who had an unknown time of ingestion, such as this patient, or those who are symptomatic should undergo flexible endoscopy for coin removal. Coins lodged >24 hours are at significant risk for complications (eg, erosion, perforation).
- Emergency bronchoscopy would be appropriate for an airway foreign body causing respiratory compromise.
Double ring sign: