genetic mutations in pulmonary hypertension
- related: pulmonary hypertension
- tags: #literature #pulmonology
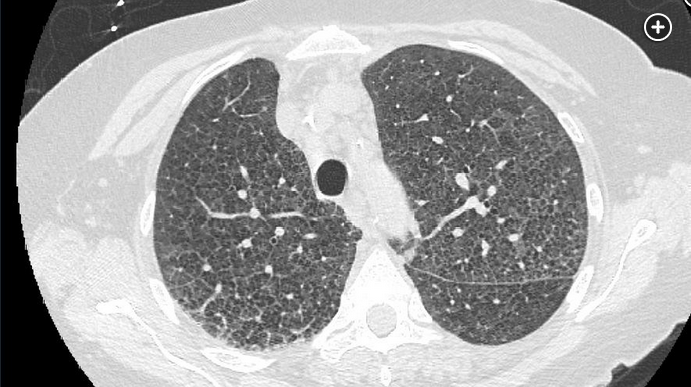
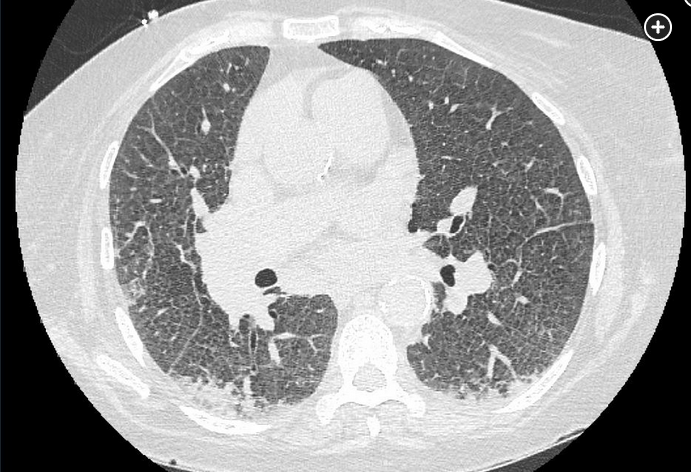
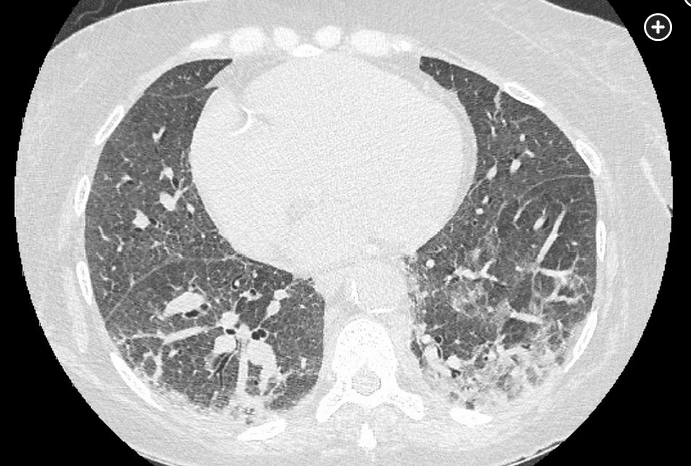
This patient presents with progressive dyspnea and lower extremity edema and has severe pulmonary hypertension in the absence of either left-sided heart disease or abnormal pulmonary function. Her chest CT scan shows diffuse intralobular and interlobular septal thickening with ground-glass mosaic attenuation; these findings are most compatible with pulmonary veno-occlusive disease/pulmonary capillary hemangiomatosis (PVOD/PCH). Mutations in the EIF2AK4 gene are associated with PVOD/PCH in up to one-third of sporadic cases (choice B is correct).
PVOD/PCH, formerly considered separate entities, is a rare cause of pulmonary hypertension that is distinct from pulmonary arterial hypertension (PAH). Compared with patients with PAH, patients with PVOD/PCH have a more fulminant course and a worse prognosis. Although unequivocal diagnosis may require surgical or autopsy pathologic examination, the diagnosis of PVOD/PCH is strongly suggested by the presence of pulmonary hypertension, pulmonary interstitial edema, intralobular and interlobular septal thickening, and ground-glass opacities in the absence of left atrial hypertension. Mediastinal lymphadenopathy, pleural effusions, and pericardial effusion may also be seen. Hemoptysis, usually nonmassive, may occur, and hemosiderin-laden macrophages are frequently seen in sputum cytology or BAL specimens.
Of note, mutations in the BMPR2 gene are most commonly seen in patients with idiopathic or heritable PAH but can occur less commonly in patients with PVOD/PCH. Likewise, the presence of EIF2AK4 mutations has been described in a small minority of patients with PAH, many with some clinical features of PVOD/PCH that appear to have been misclassified. Differentiation of PVOD/PCH from PAH is important because medications used to treat PAH, such as epoprostenol, can precipitate life-threatening pulmonary edema in a subset of patients with PVOD/PCH.
Endoglin is a membrane glycoprotein that is part of the transforming growth factor-β complex. It plays a critical role in angiogenesis, and mutations in the ENG gene are associated with the development of hereditary hemorrhagic telangiectasia, formerly known as Osler-Weber-Rendu syndrome (choice A is incorrect).
The EGFR gene encodes a transmembrane receptor for the epidermal growth factor family of peptide ligands. EGFR mutations that lead to overexpression are associated with adenocarcinoma of the lung and other malignancies and present a therapeutic target for tyrosine kinase inhibitor drugs such as erlotinib, afatinib, and osimertinib (choice C is incorrect).
Folliculin is the protein product of the tumor suppressor gene FLCN and has a variety of functions, including regulation of the Akt/mammalian target of rapamycin pathway. Mutations in FLCN are associated with Birt-Hogg-Dubé syndrome, which is characterized by cystic lung disease, fibrofolliculomas, and kidney tumors (choice D is incorrect).