histoplasmosis
- related: Infectious Disease ID
- tags: #literature #pulmonology
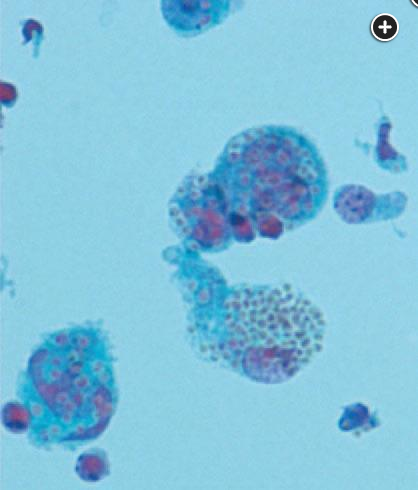
Grocott’s Methenamine Silver (GMS) stain of the lung showing histoplasmosis.
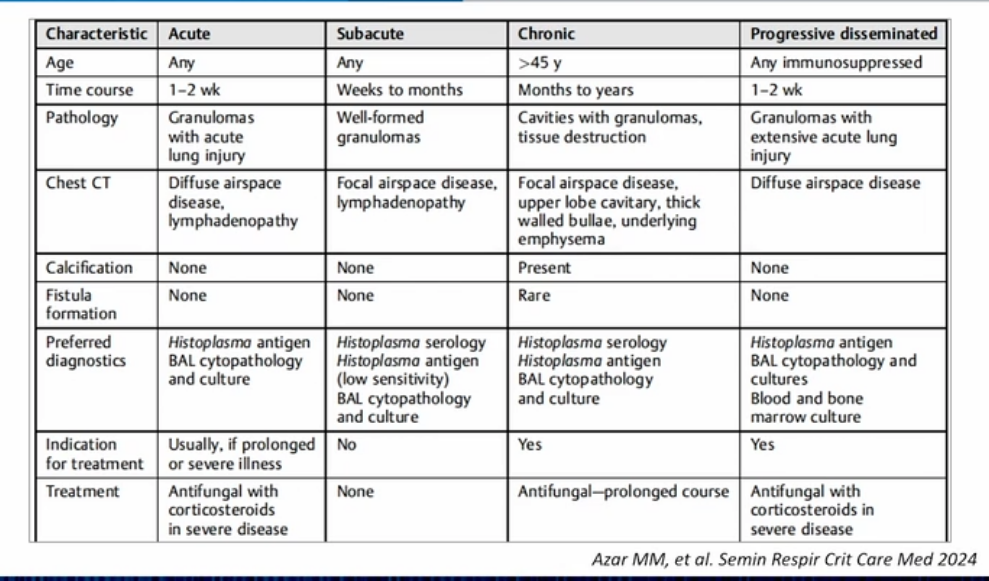
- 4 phases of disease
- acute: looks like pna
- subacute: usually see in clinic
- chronic: not too much sx but pulmonary nodules or cavities
- disseminated: immunocompromised
Pathogenesis
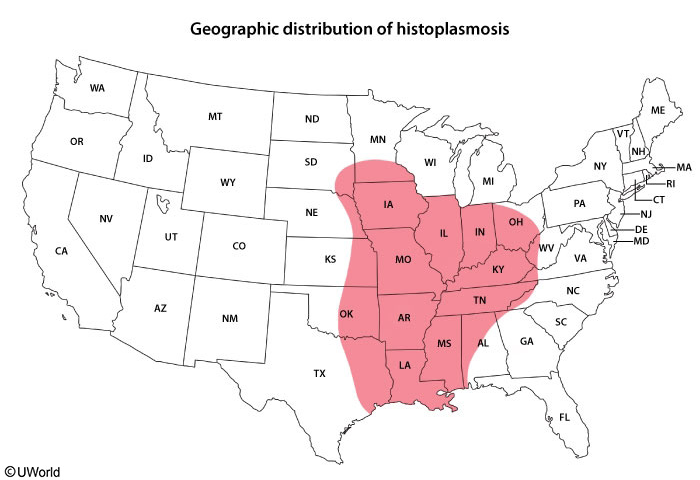
Histoplasma capsulatum is responsible for one of the most common endemic mycoses in the world. Acquired by inhalation of airborne conidia, this organism primarily produces asymptomatic pulmonary infection. It is distributed along the Mississippi River Valley (Ohio, Missouri, Indiana, Mississippi) in the United States, in Central and South America, in the Caribbean, and in regions of Africa, Australia, and India.
Symptoms
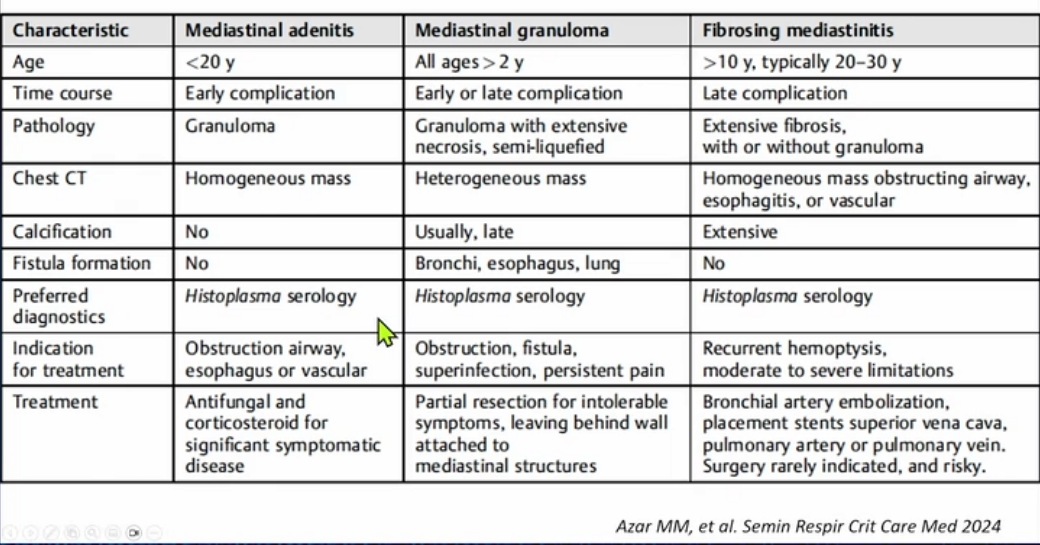
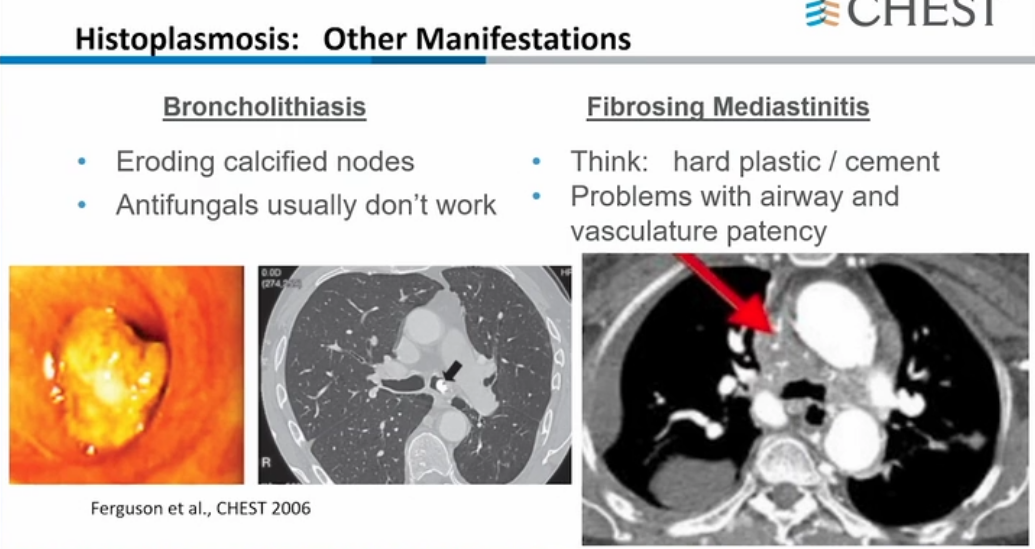
Histoplasmosis most commonly presents with acute respiratory symptoms. Other presentations, in declining order of frequency, include asymptomatic infection, disseminated infection, chronic pulmonary symptoms, rheumatologic symptoms, pericarditis, and sclerosing mediastinitis.
Diagnosis
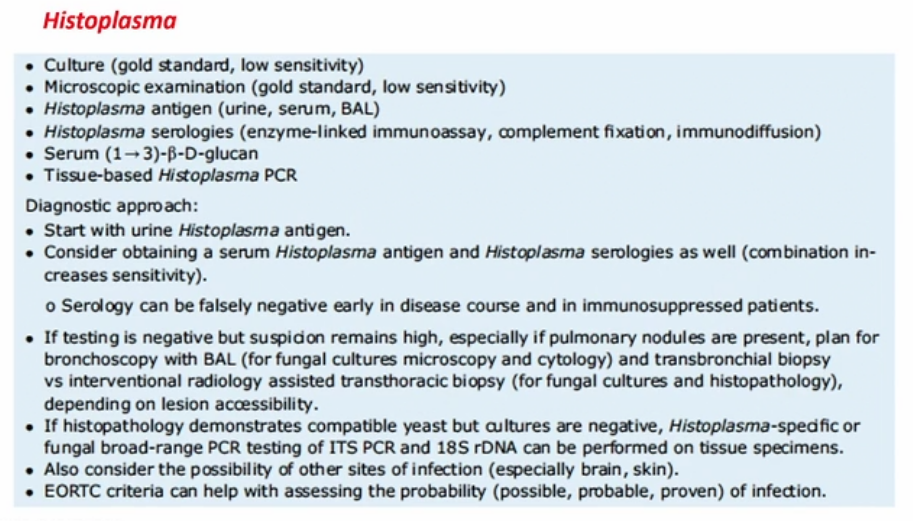
The Histoplasma urinary antigen assay has a sensitivity and specificity of greater than 85% in acute and disseminated infection but less than 50% in chronic infection. Identification of the fungus by tissue culture can be a lengthy process but is indicated for clinically suspected cases in which the urinary antigen assay result is negative.
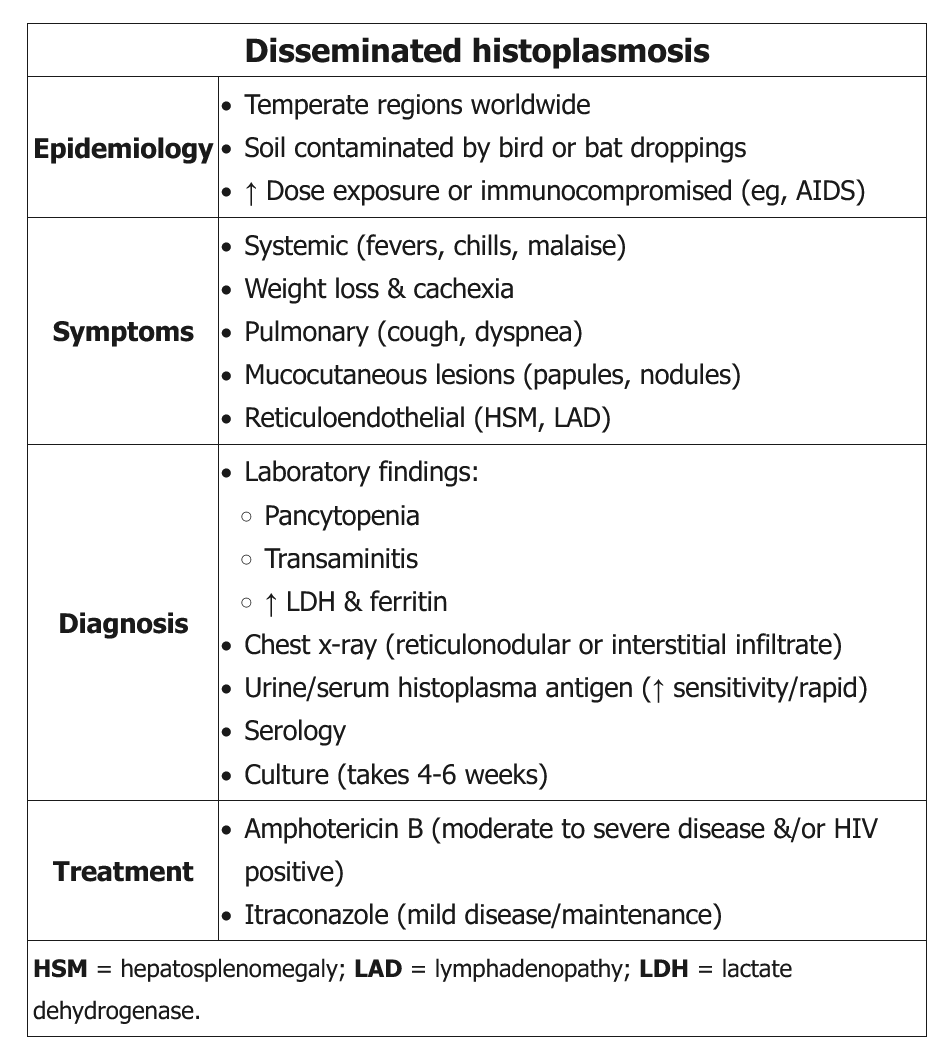
- histoplasmosis should be suspected in HIV patients due to reduced cell-mediated immunity
- disseminated histoplasmosis leads to sepsis, pancytopenia, adrenal insufficiency, and lymphadenopathy
- urine antigen cross reacts with histo/blasto but doesn’t have high sensitivity.
- Can have high LDH and mimics PCP
Treatment
- asymptomatic and mild histoplasmosis does not require treatment
- treat moderate to severe histoplasma with amphotericin B and itraconazole