increased delta P is sign of increased clotting on ECMO
- related: ECMO extracorporeal membrane oxygenation
- tags: #literature #icu
Delta P is membrane pressure drop, also AKA transmembrane pressure, defined by difference in pressure of blood pre-membrane (ecmo) lung and post-membrane lung.
Normal delta P should be <50.1 P usually increases with time on ECMO. Gradual increase in P is expected as result of fibrin accumulation..2 Increased pressure could indicated proper anticoagulation or oxygenator replacement.1
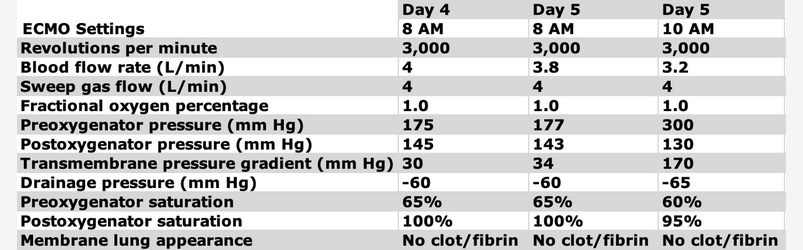
Sudden change in transmembrane pressure can indicate membrane lung failure (usually from clot) and requires emergent exchange of membrane lung. E.g.:
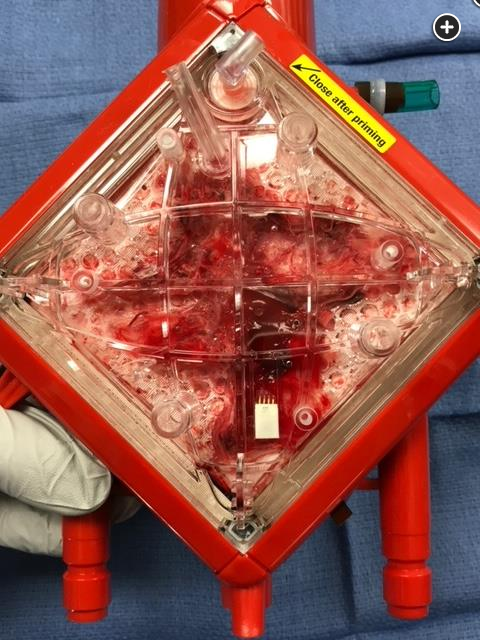
- Membrane lung demonstrating clot after circuit is washed out.
In venovenous (VV) ECMO, the membrane lung is responsible for respiratory gas exchange (oxygen uptake and carbon dioxide removal). Monitoring membrane lung function can be divided into three categories: (1) hematologic variables (hemolysis and coagulopathy), (2) pressure monitoring, and (3) membrane lung gas transfer (Figure 4). Worsening oxygenation during support with VV-ECMO should prompt the intensivist to assess membrane lung function.
The presence of clot and fibrin on the membrane lung (Figure 5) can be a sign of impending membrane lung failure and the potential need to change out a membrane lung. Likewise, an increase in the transmembrane pressure gradient may indicate clot formation within the oxygenator. If an elevated transmembrane pressure (normal, <50 mm Hg) is noted, one should check the postoxygenator blood gas to calculate oxygen transfer across the membrane lung. The absence of visual clot or fibrin on the lung membrane does not mean the membrane lung does not need to be exchanged.
Most often, there are signs of impending membrane lung failure allowing for an elective and controlled exchange. This case did not have signs before the acute membrane failure, leading to an emergent exchange. Ideally, this should be emergent yet coordinated across the multidisciplinary team caring for this patient. During a membrane lung exchange, one team member cares for the patient (eg, optimizes mechanical ventilation, ensures hemodynamic stability) while the other team members manage the ECMO circuit and membrane exchange.3456
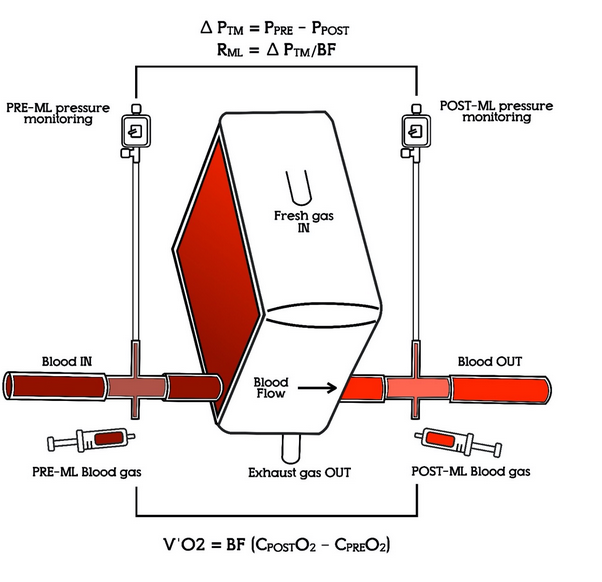
“The pressure drop (ΔP) is calculated as the difference between the preand the post-ML pressure. The resistance within the ML, RML, can be trended as ΔP/circuit blood flow rate (BFR). Oxygen transfer (V’O2) across the ML can be obtained from blood gas analysis as the product of BFR and the difference in oxygen content between the postand pre-ML (CPostO2 – CPreO2).” ML = membrane lung.6
Links to this note
Footnotes
-
http://icuroom-futurearchive2.blogspot.com/2019/04/delta-p-on-ecmo.html ↩ ↩2
-
Badulak JH. Venovenous extracorporeal membrane oxygenation. Flow, pressure, hematology, and emergencies. ATS Sch. 2020;2(1):138-139. PubMed ↩
-
Patel B, Arcaro M, Chatterjee S. Bedside troubleshooting during venovenous extracorporeal membrane oxygenation (ECMO). J Thorac Dis. 2019;11(suppl 14):S1698-S1707. PubMed ↩
-
Zakhary B, Vercaemst L, Mason P, et al. How I approach membrane lung dysfunction in patients receiving ECMO. Crit Care. 2020;24(1):671. PubMed ↩ ↩2