Namen hypoventilation syndrome 2025
Conditions and Challenges
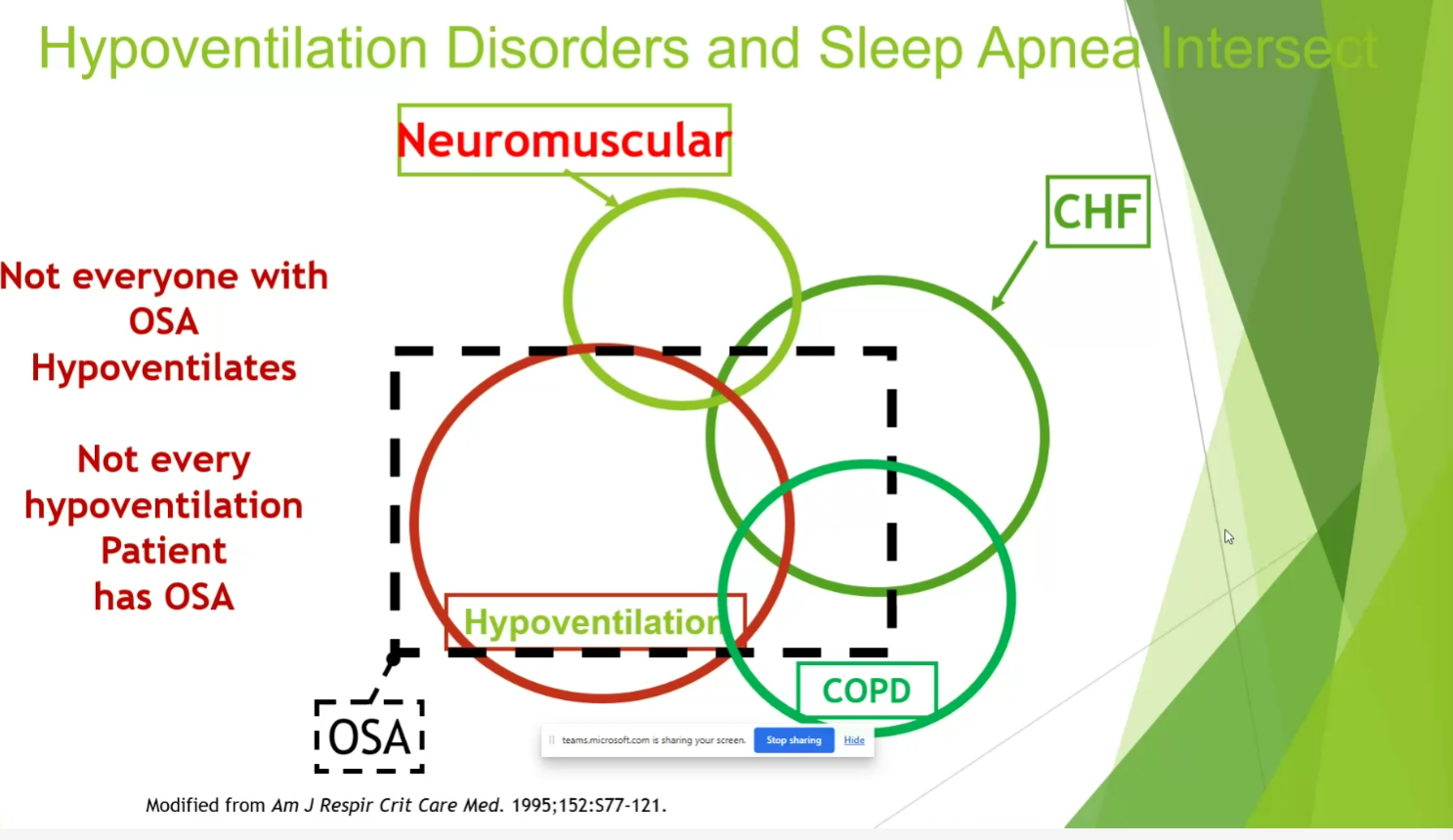
- up to 40% CHF, 15-20% NMD, up to 50% COPD, most of OSA
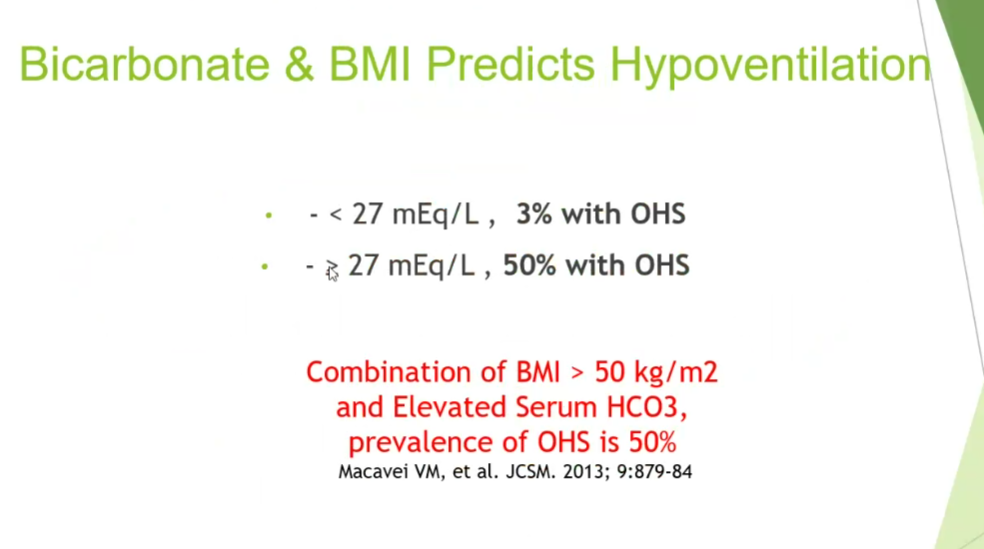
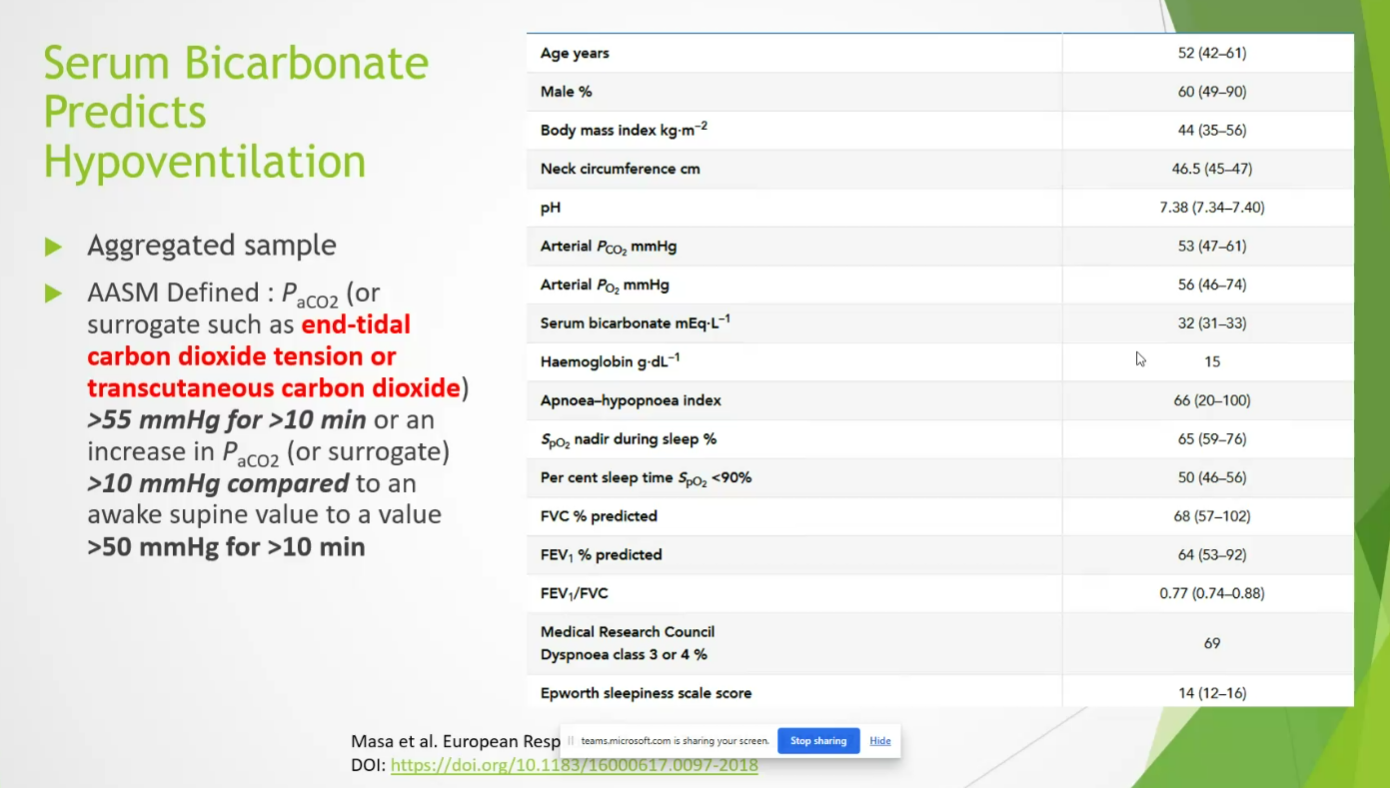
- bicarb predicts in pts with elevated BMI
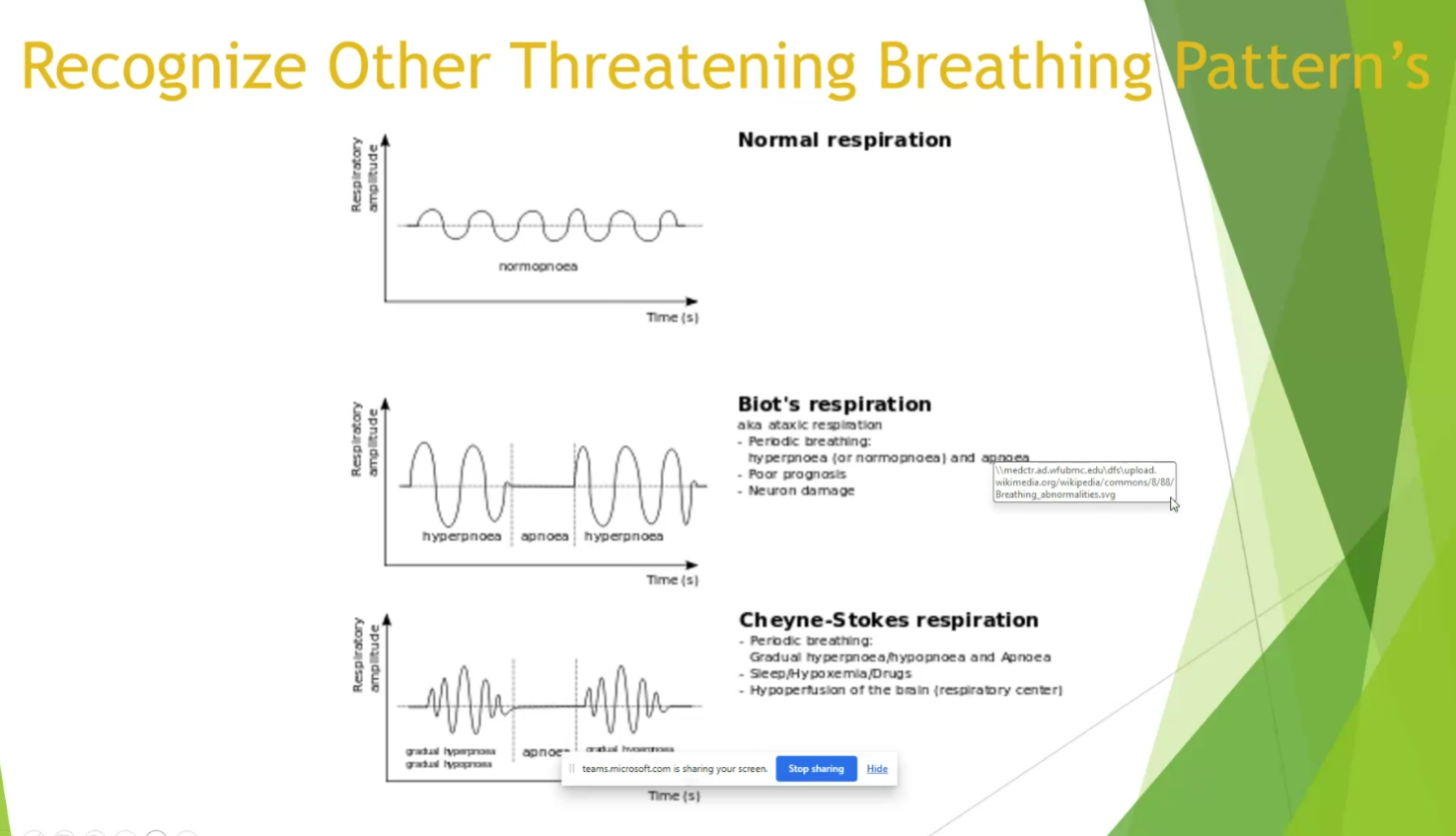
- ataxic breathing
- central pauses can become as long as 2-3 min with agonal breathing
- often in opioid users
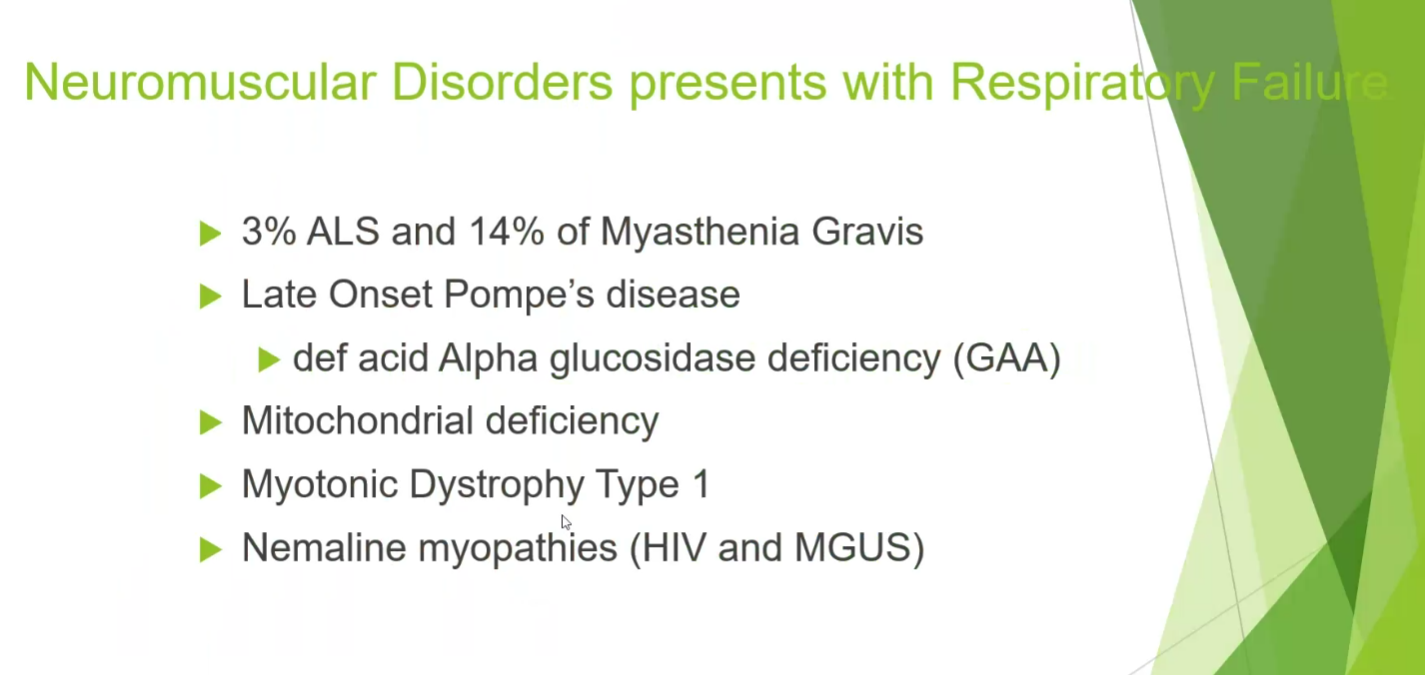
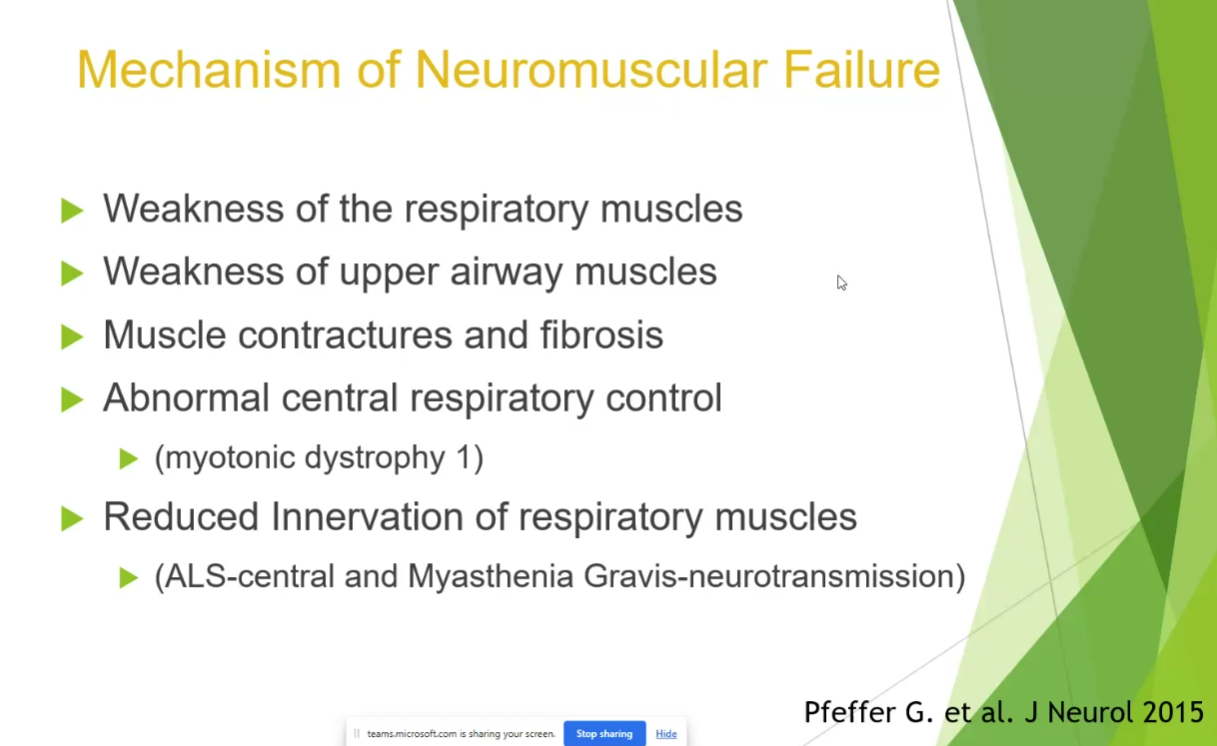
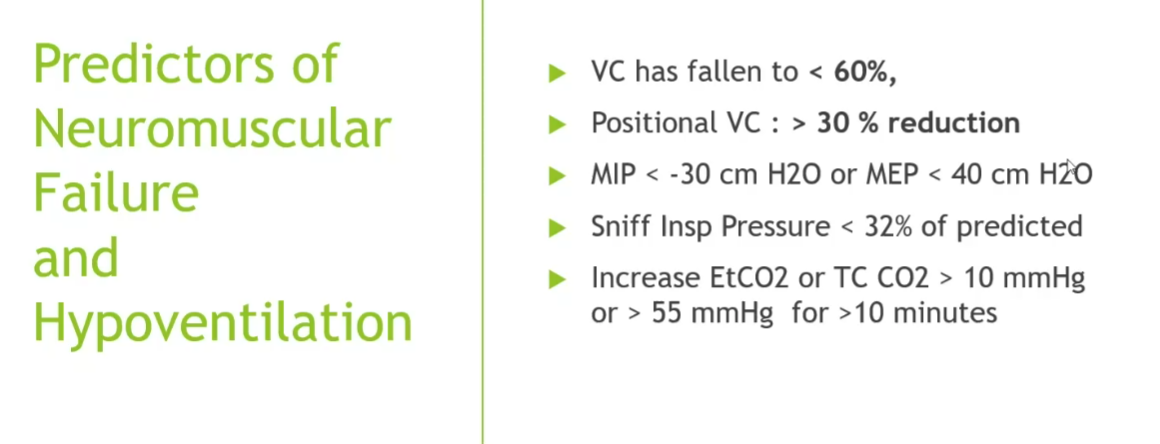
Neuromuscular disorders
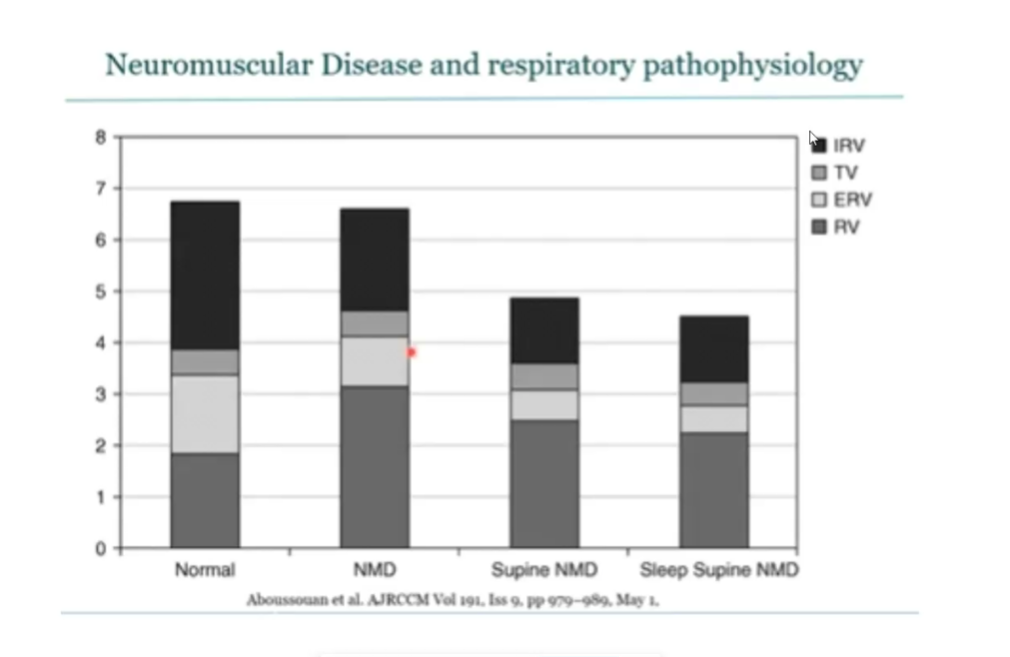
- laying flat can show dramatic drops
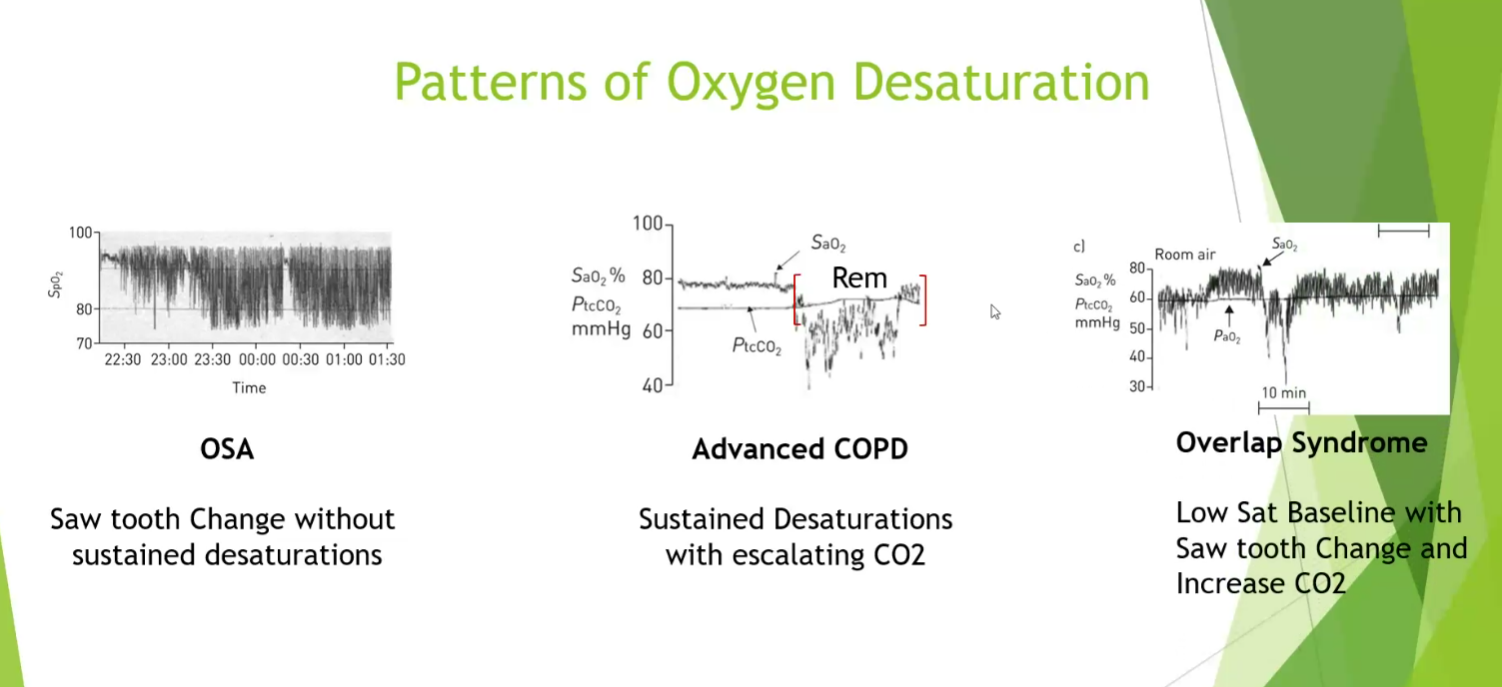
- OSA: quick drops and recovery
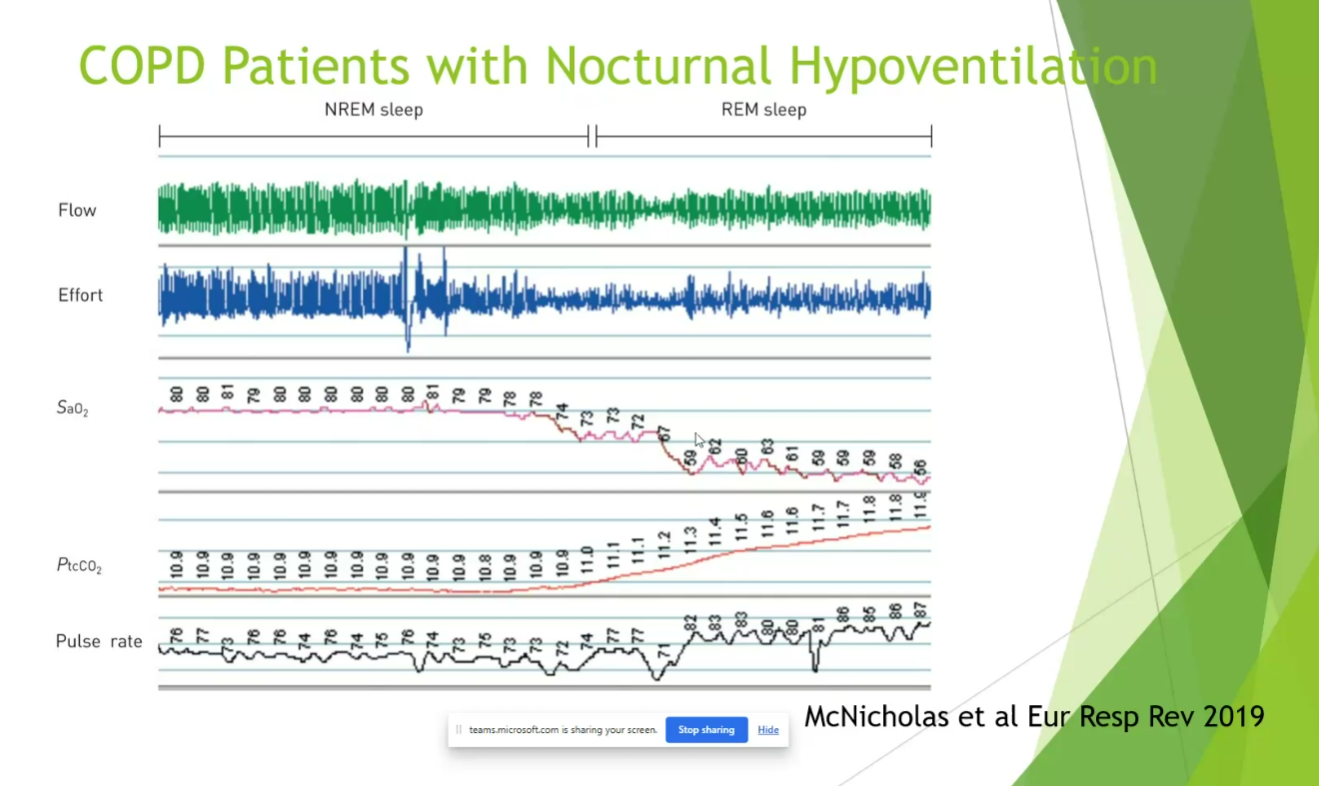
- COPD: sustained desat with CO2 go up
- Combined: dramatic changes in both CO2 and desat
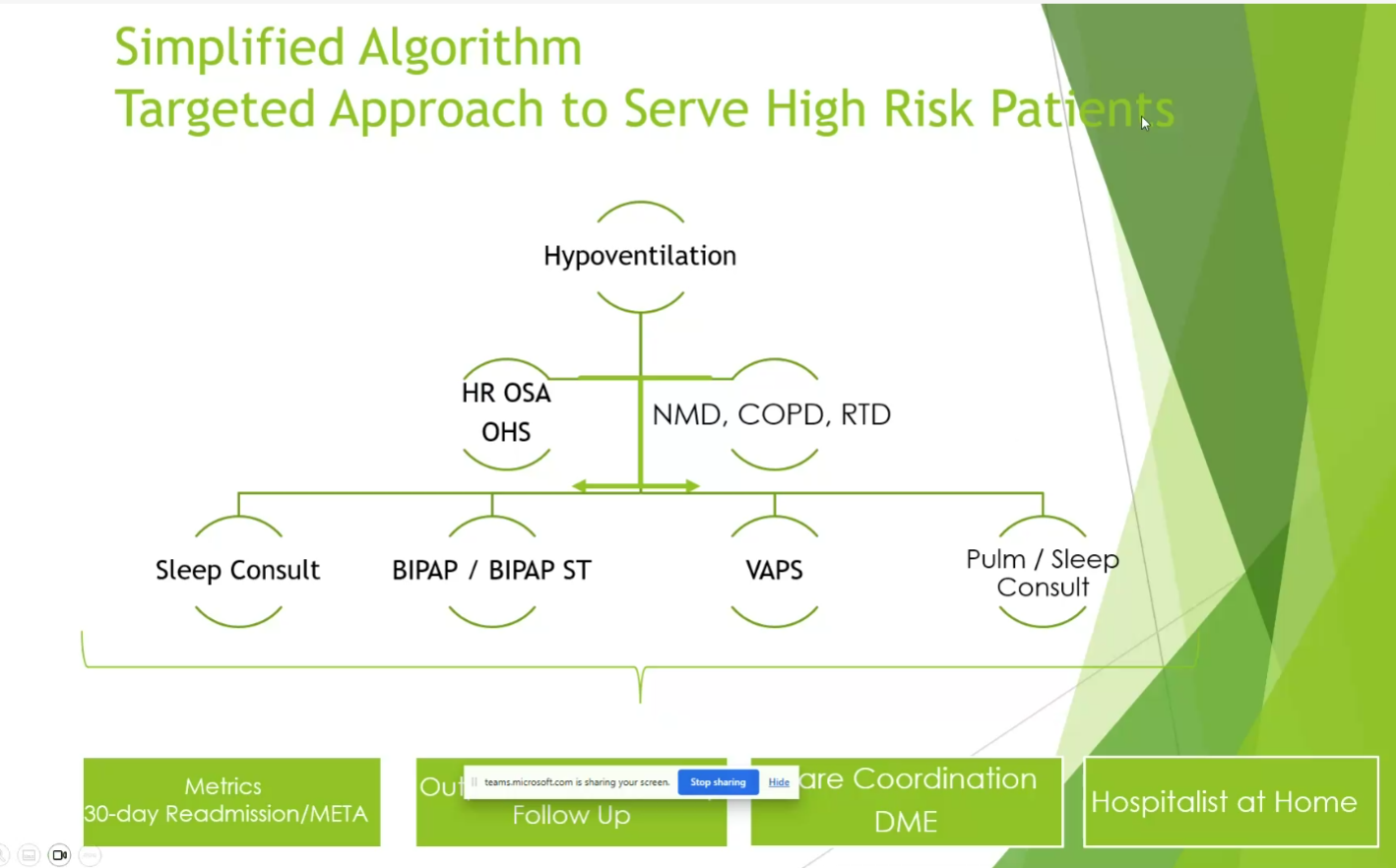
- not every needs NIV
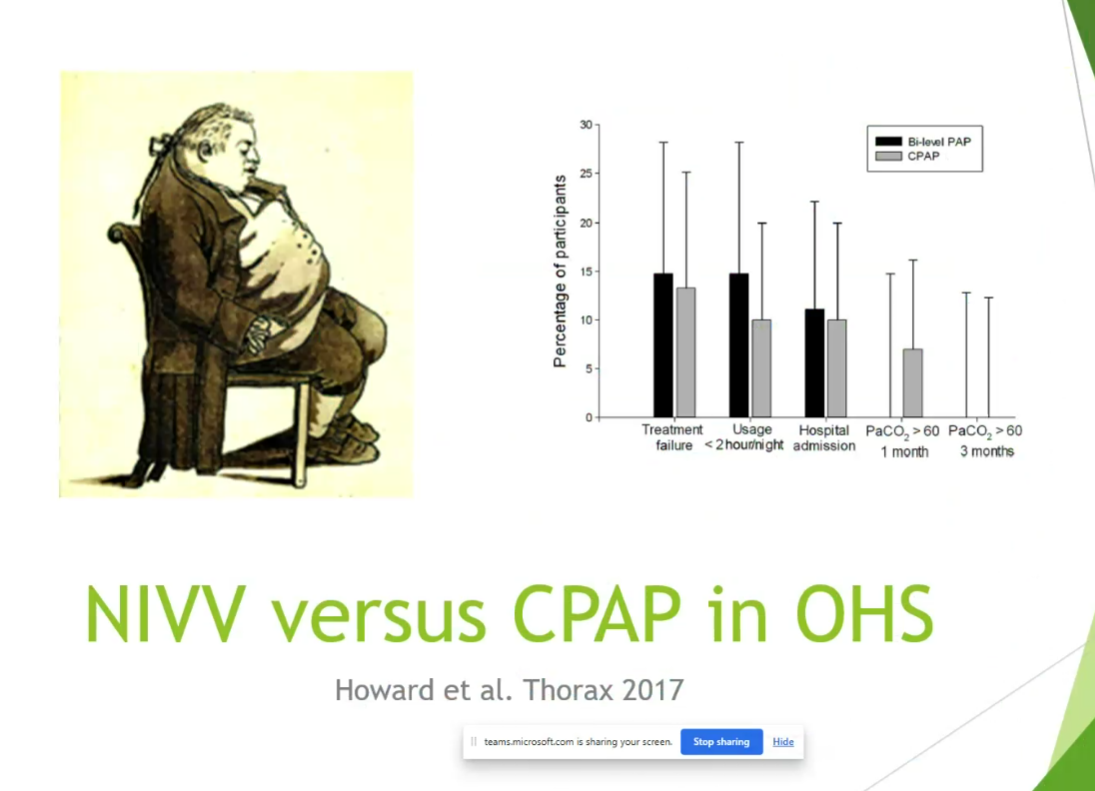
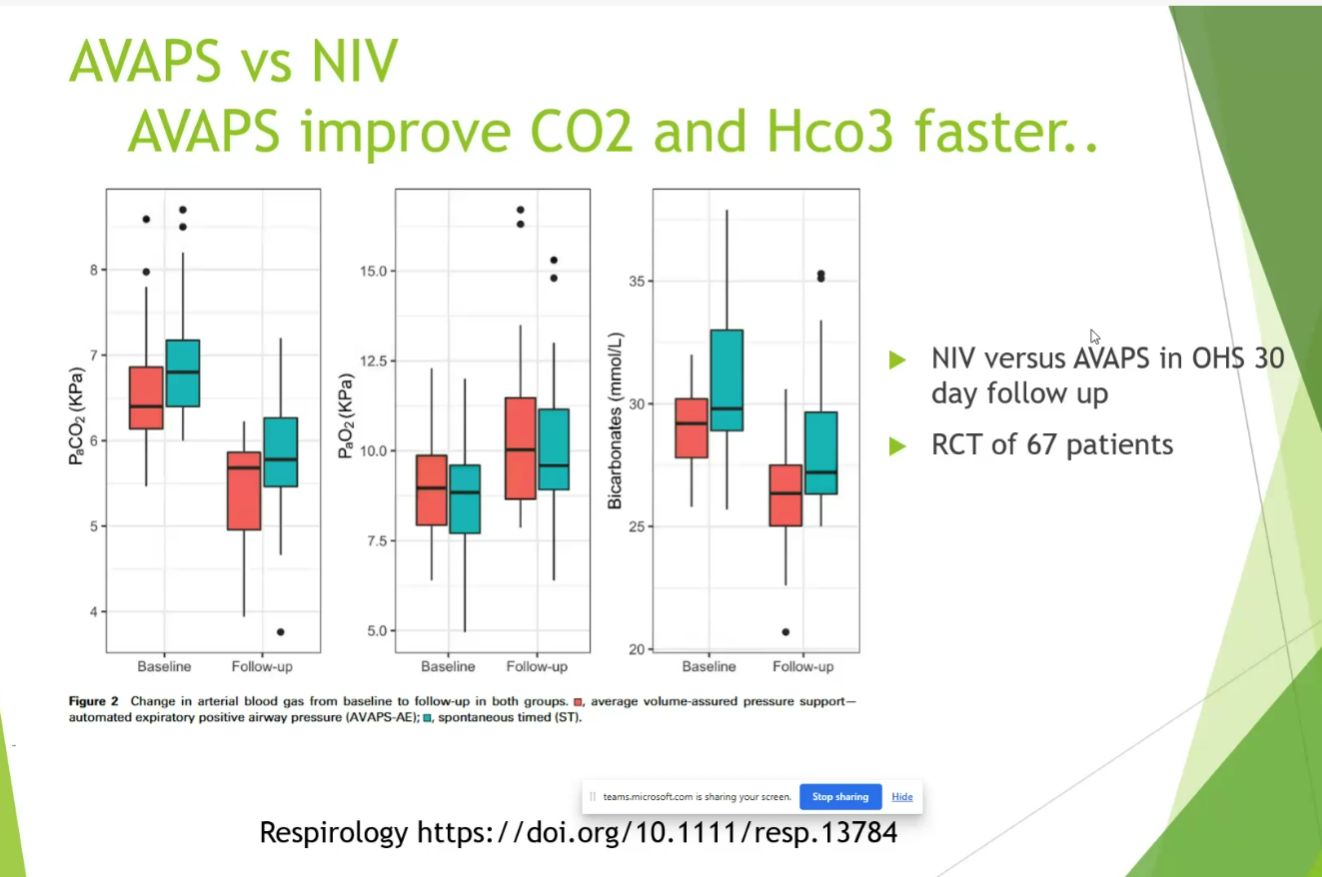
- CPAP effective in a lot of cases, will improve CO2 but not as fast as Bipap.
- CPAP can treat OHS with elevated CO2 if stable
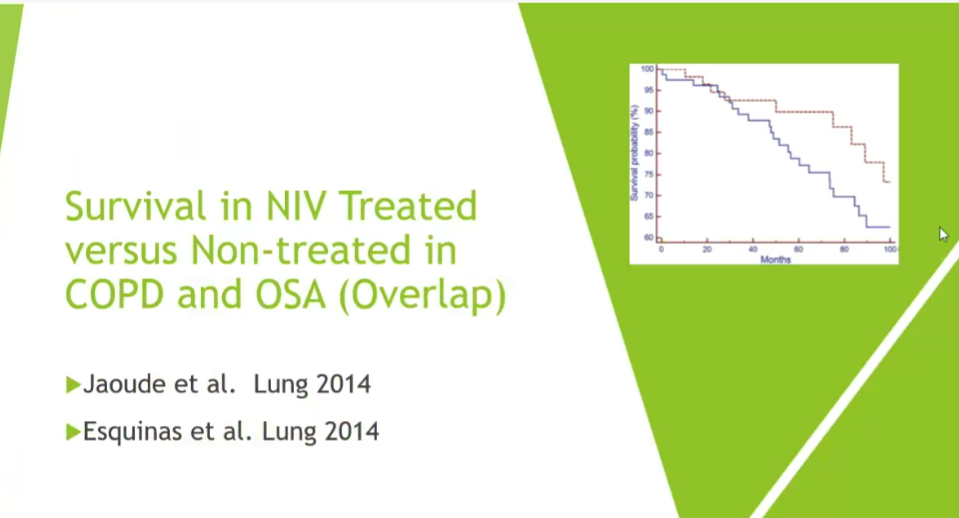
- survival in NIV treated groups is higher with NIV when there is overlap
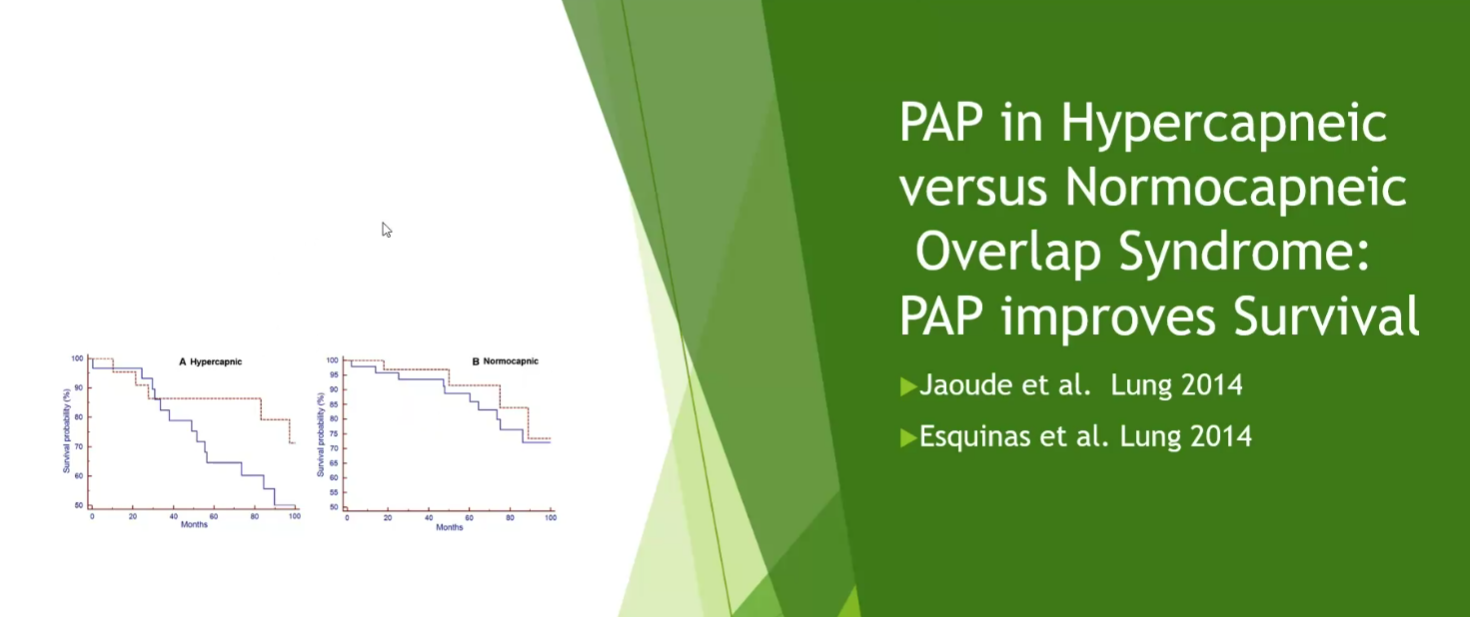
- normocapneic patient doesn’t receive as much benefit from bipap
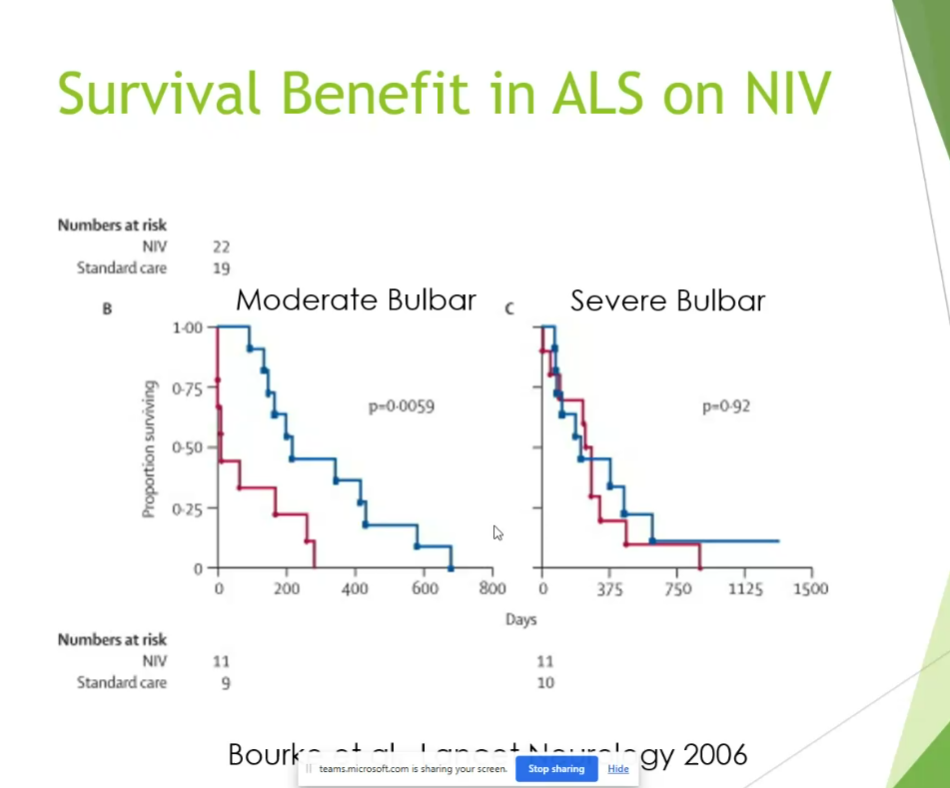
- ALS pts with severe bulbar symptoms don’t benefit as much
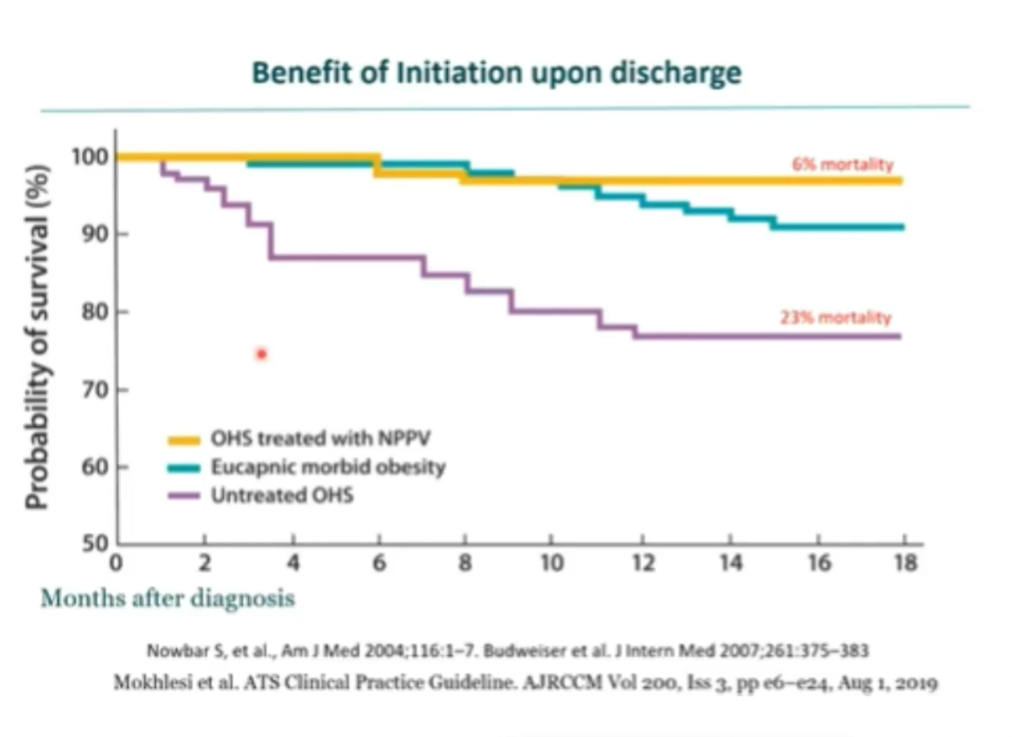
- reduction in mortality less so in eucapnic morbid obesity

- correcting CO2 maximally even shows benefit
Monitoring

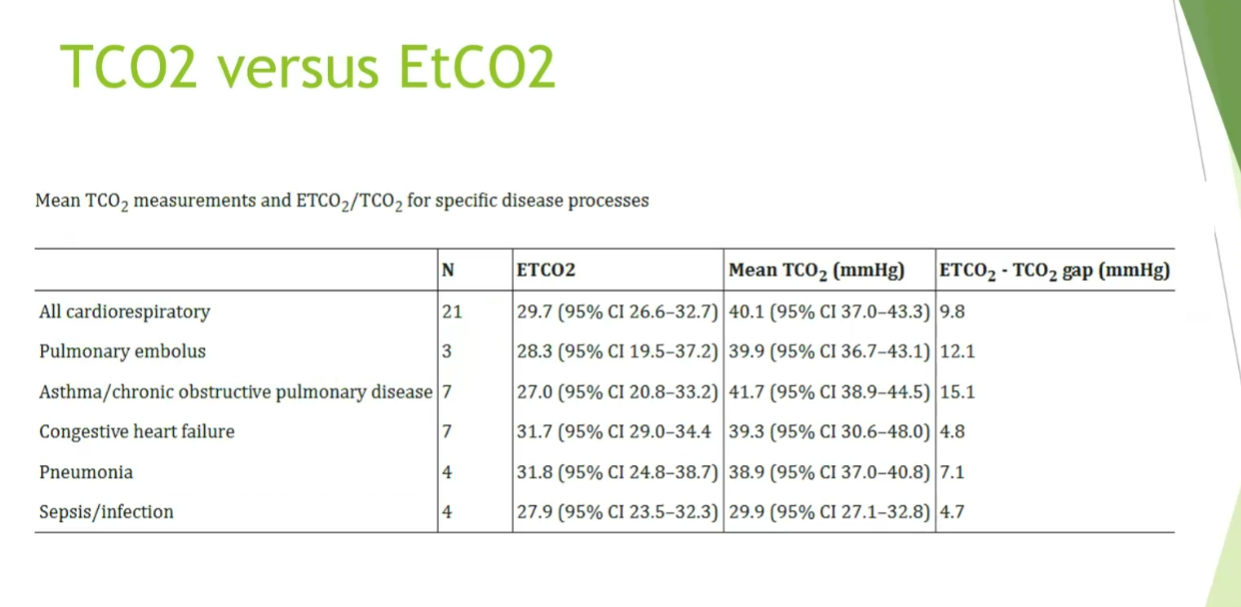
- mean co2 and tCO2 can be quite different between different conditions
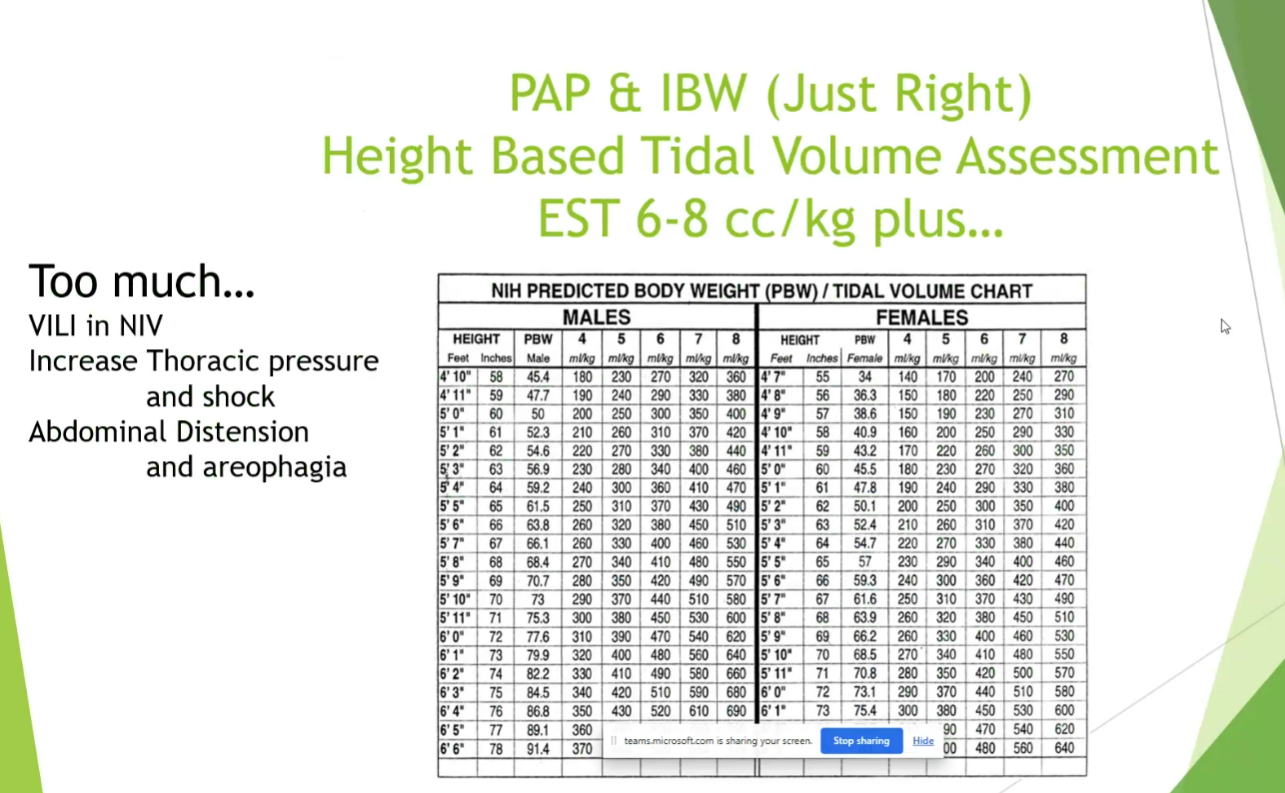
- pressure based on TV
- intestinal obstruction: should probably not do NIV if they don’t have NG in place
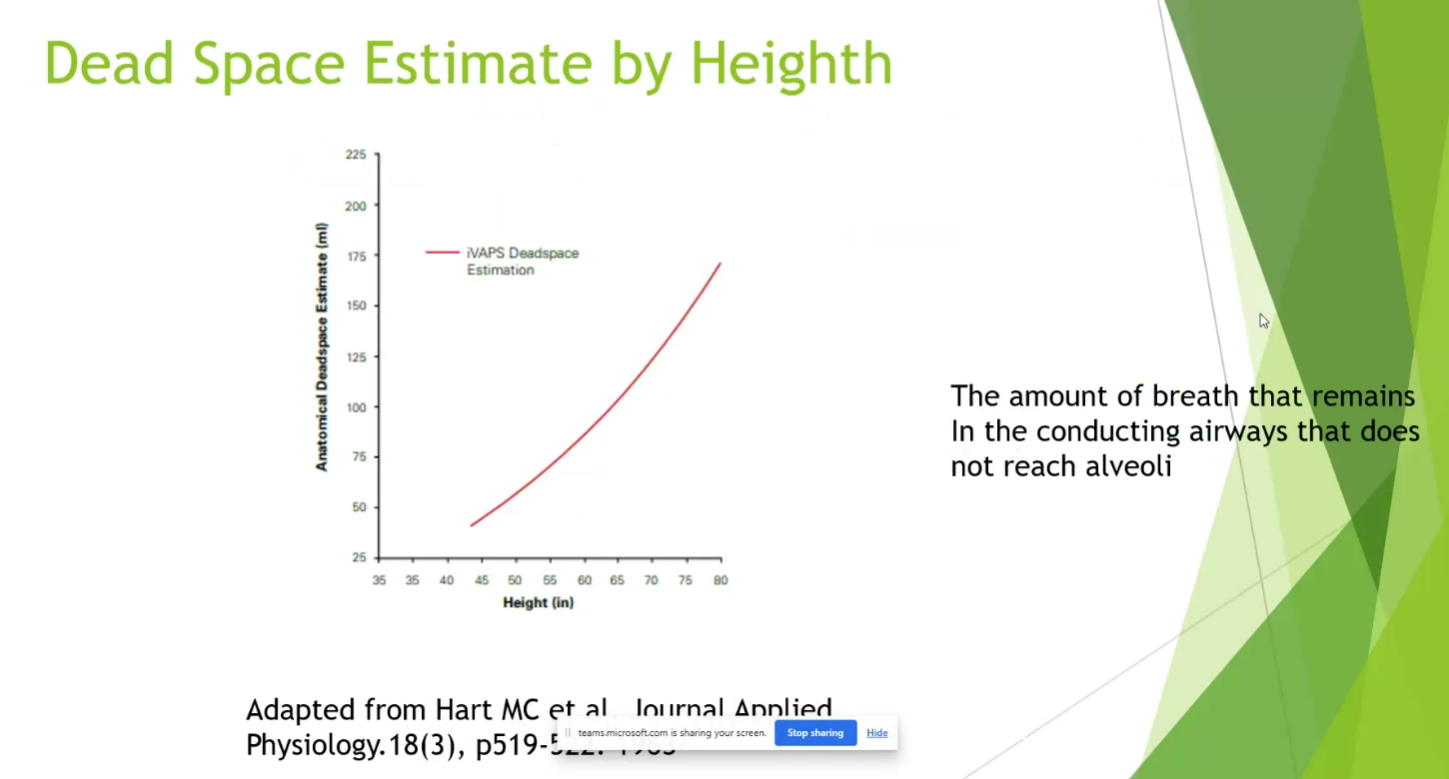
- 6-8 cc/kg + patient’s dead space (around 150cc) should be upper limit target of TV
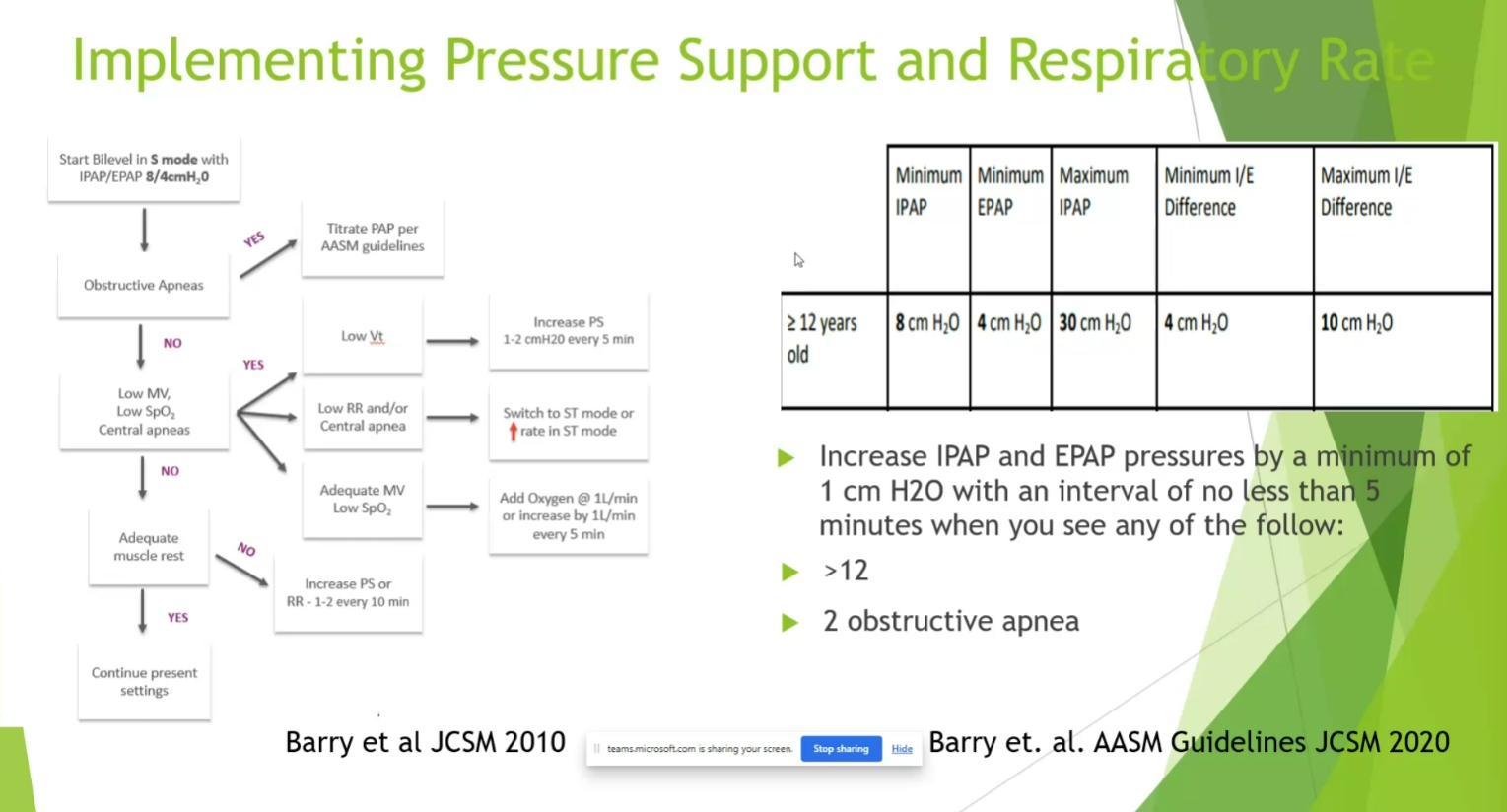
- BMI over 30: start EPAP of 8 or 10 to overcome upper airway obstruction
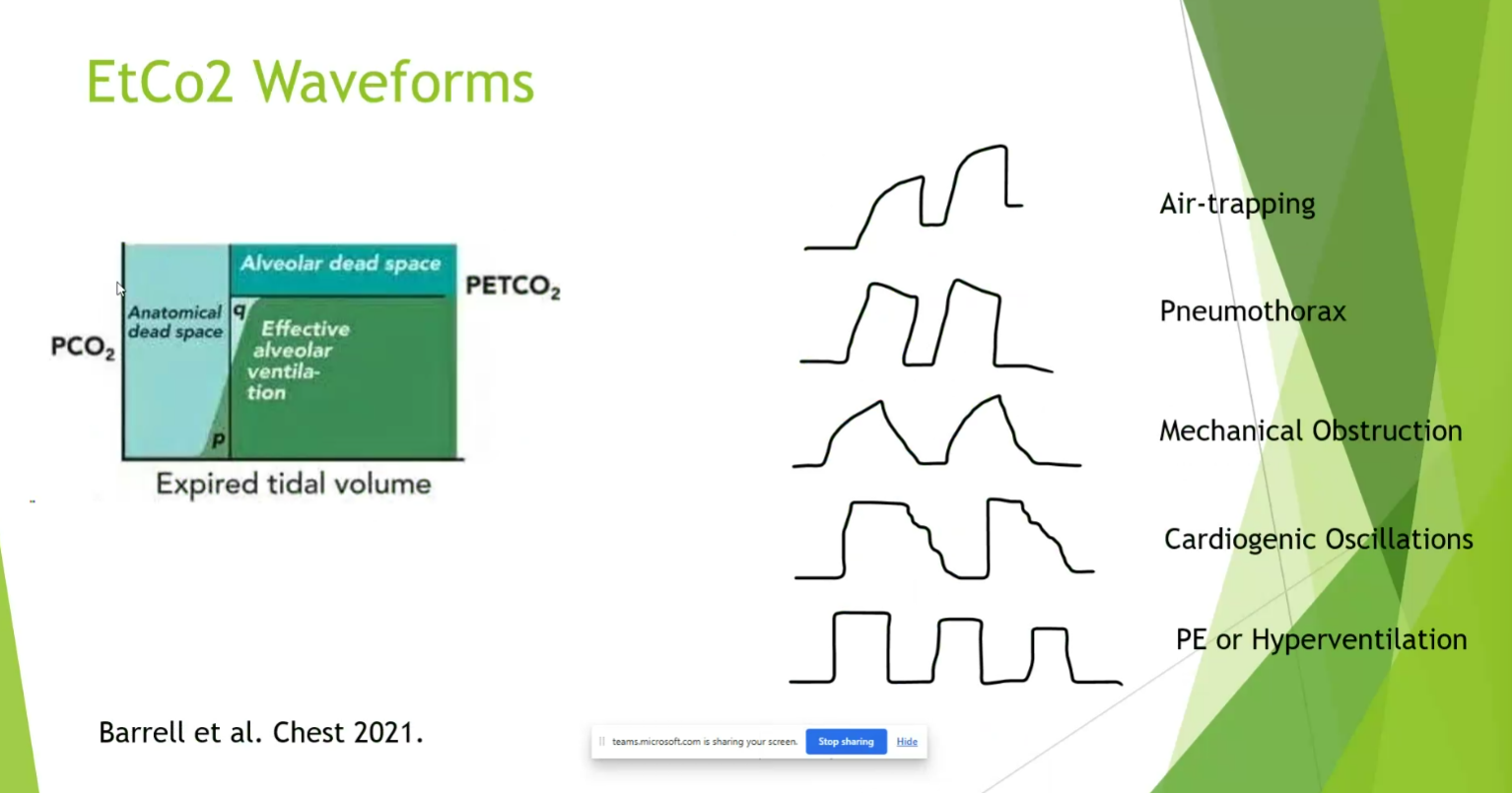
- look at flow loop to make sure there’s no obstruction on inspiratory flow loop

- no dramatic change from NIV with AVAPS
- Drift: lower and lower PS to assure tidal volume with AVAPS. Trilogy/AVAPS bug that can cause recurring admission
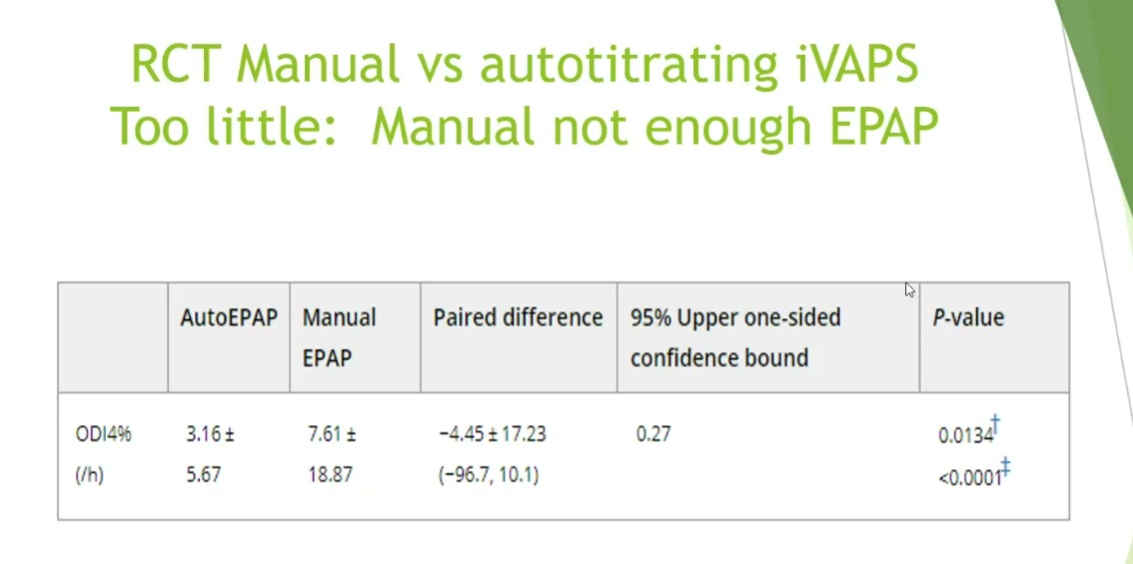
- AVAPS gets patient to PEEP faster than trained technicians at night in NMD, COPD, OHS
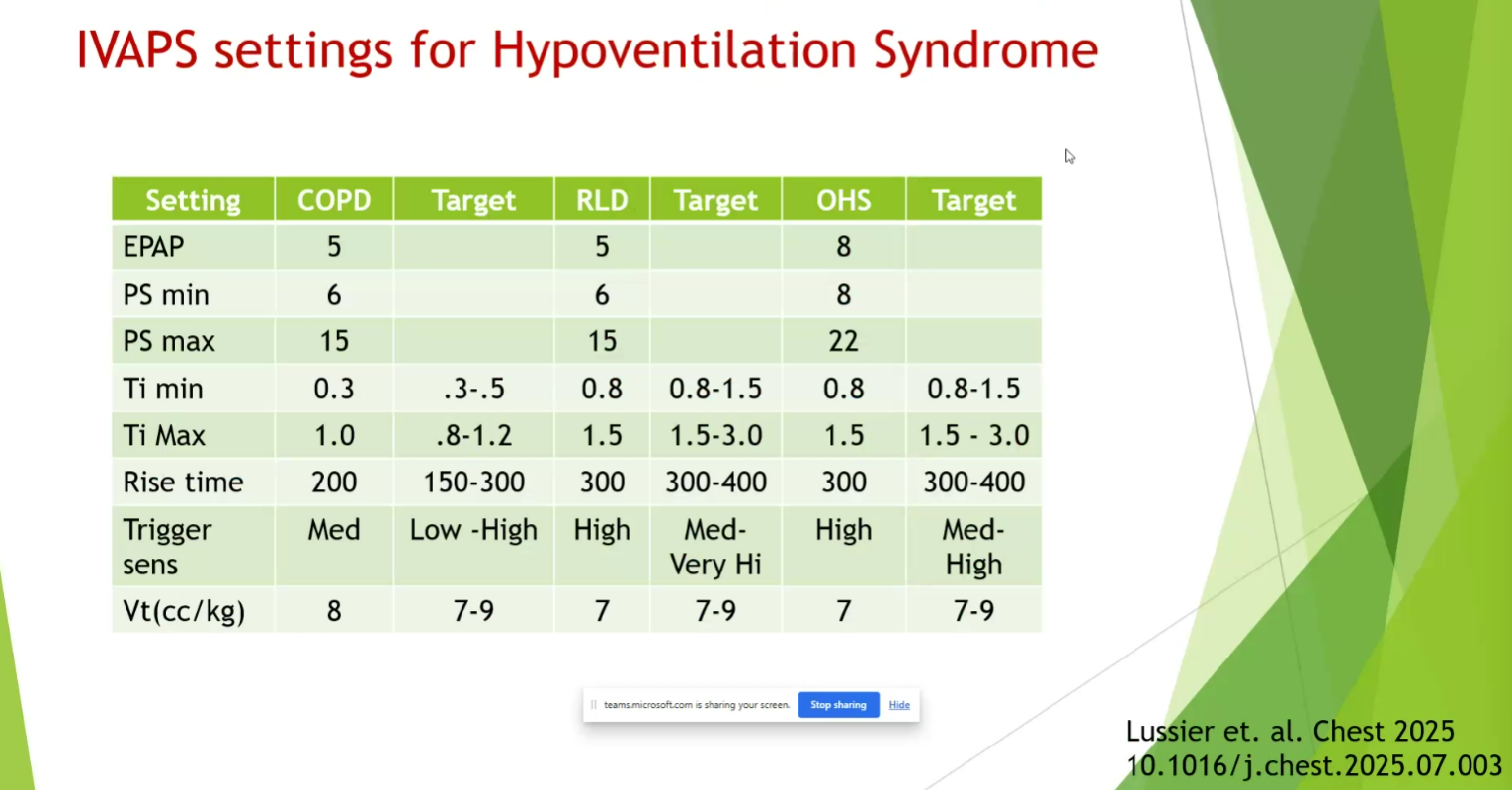
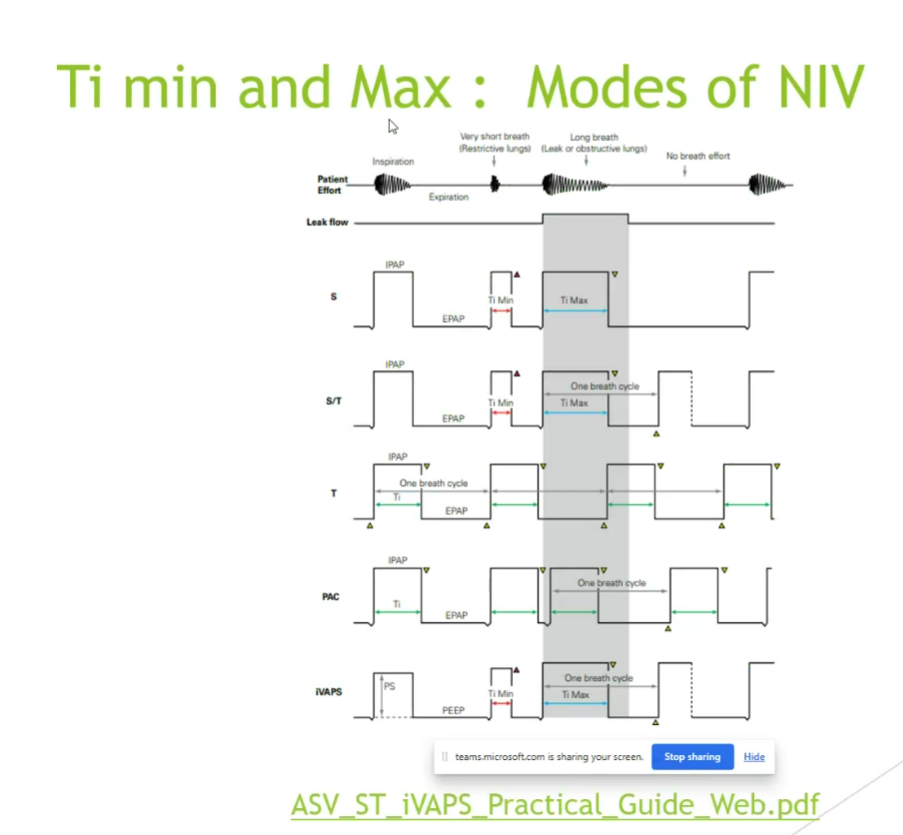
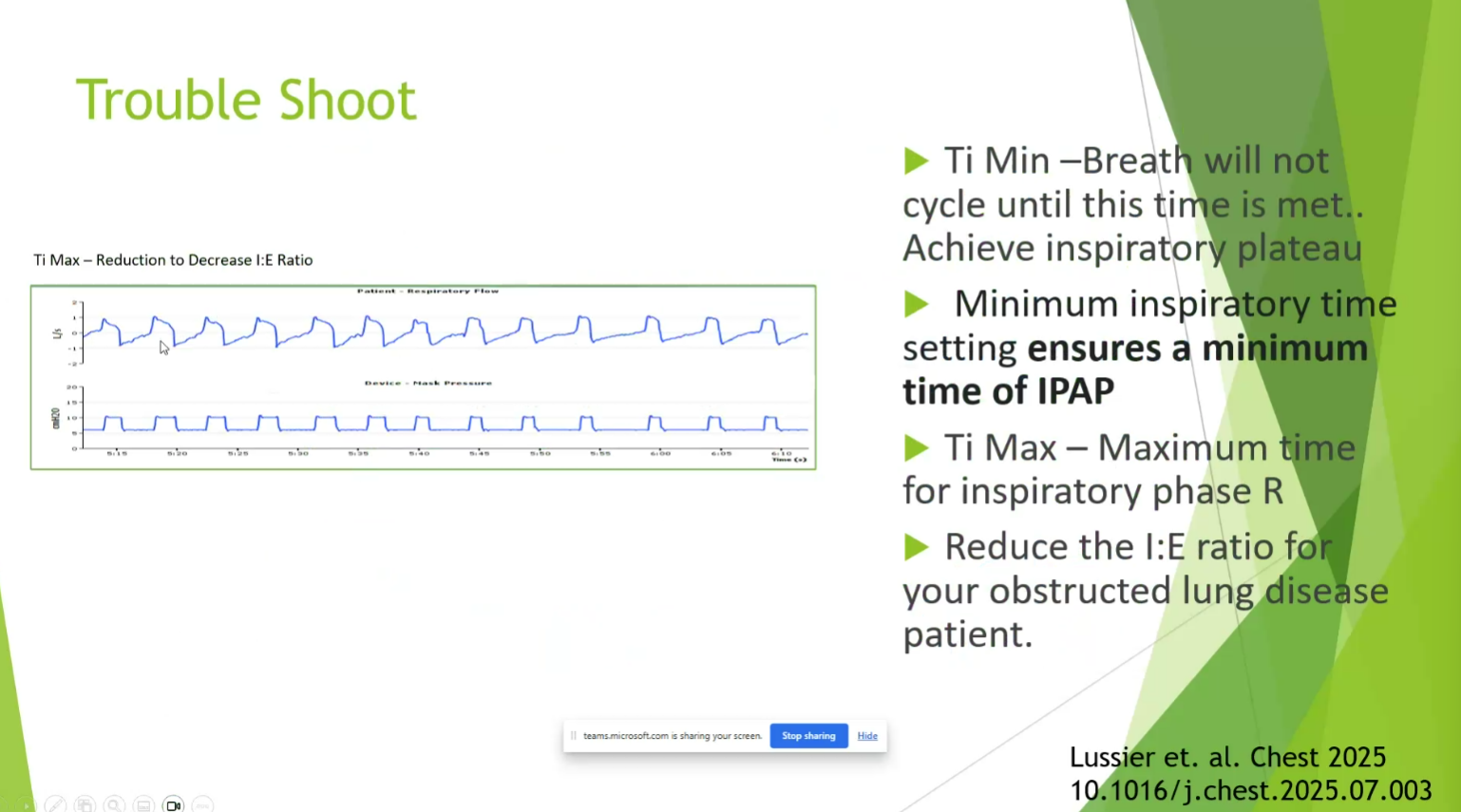
- RLD and OHS: really extend Timin and Timax for diaphragmatic support. Get TiMax to 15
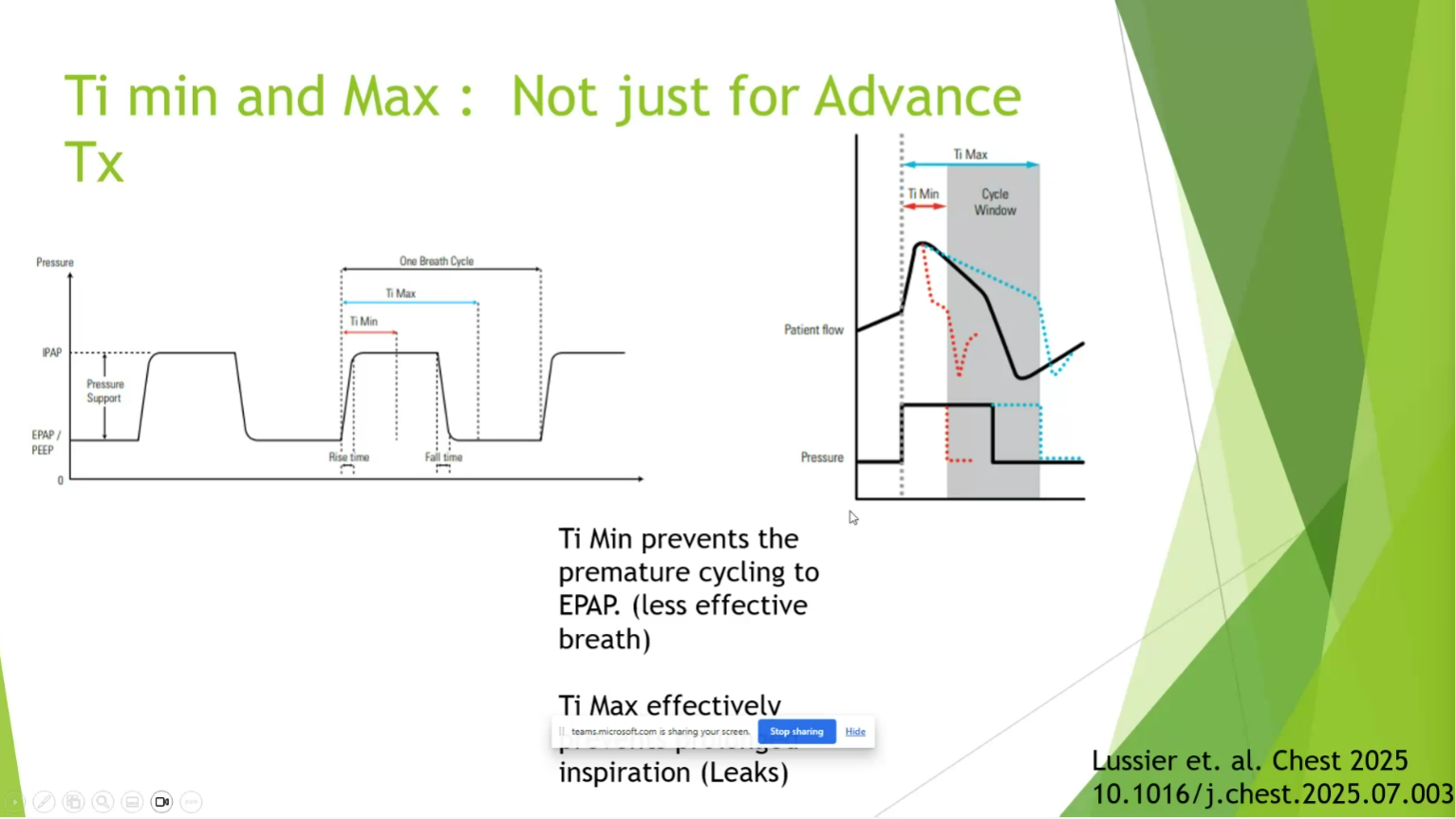
- Ti min prevents premature cycle
- Timax prevents inspiration leaks?
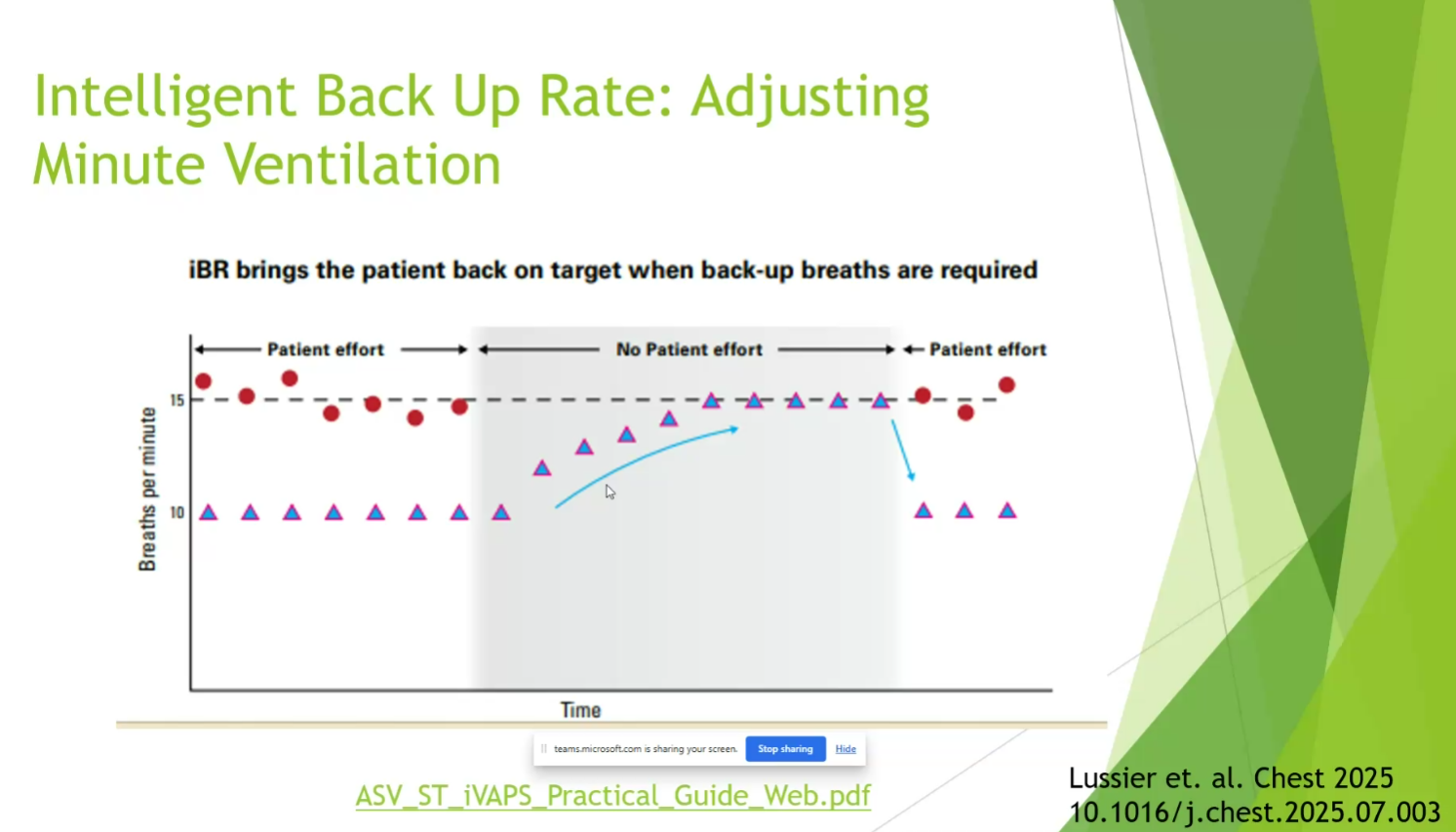
- once pressure target exceeded, respiratory rate then is increased
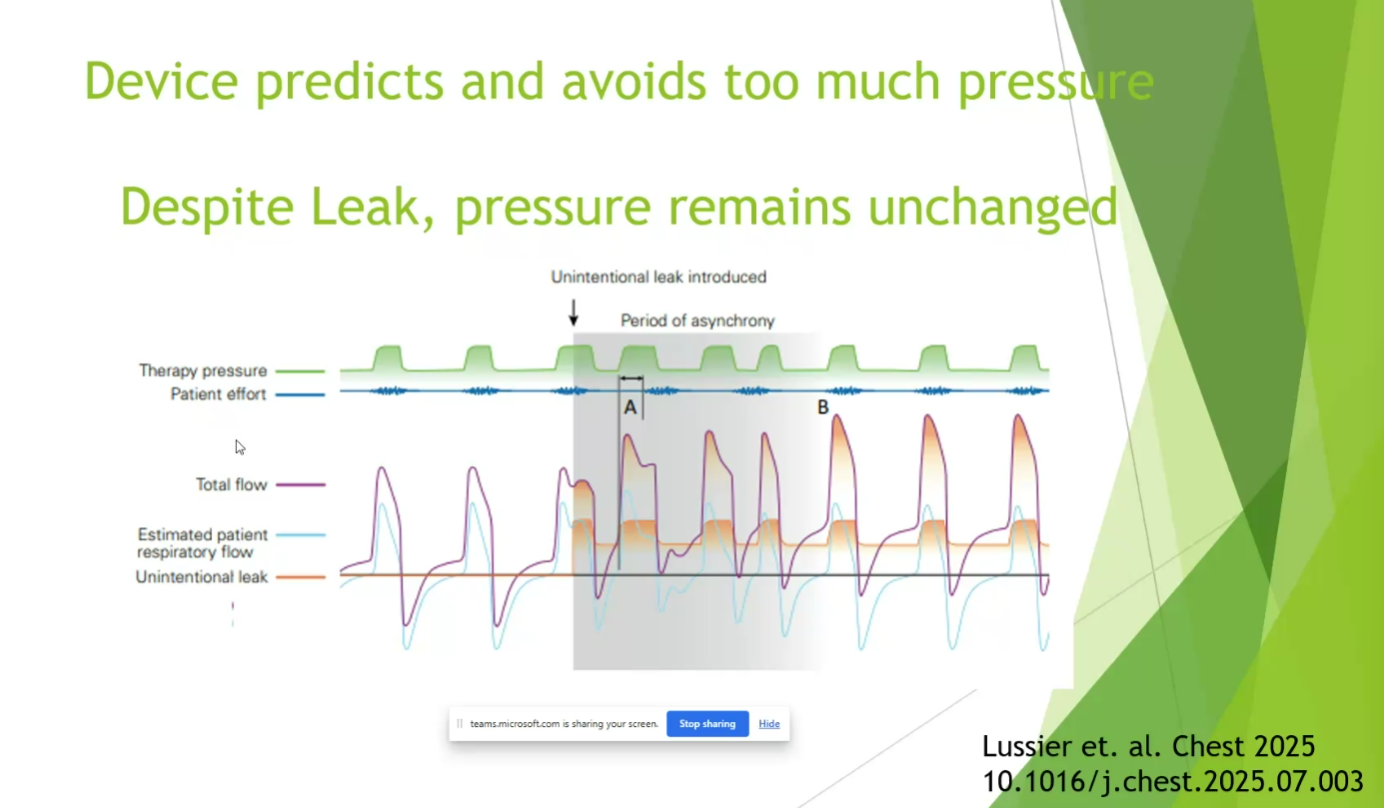
- new technology is better at adjusting pressure to not exceed pressure target with mask leaks
- send pts home with Astral devices, IVAPS
Links to this note