narcolepsy type 1 and 2
- related: Psychiatry, Sleep and Sleep Disordered Breathing
- tags: #literature #pulmonology
Narcolepsy is characterized by excessive daytime sleepiness leading to “sleep attacks” where patients suddenly fall asleep at inappropriate times. Cataplexy is a unique finding of narcolepsy, where sudden loss of muscle tone is precipitated by emotion or surprise. Sleep paralysis is also indicative of narcolepsy, and is a phenomenon in which patients temporarily feel “frozen” upon waking.
Patients with narcolepsy may experience hypnagogic (just before sleeping) and hypnopompic (occur during awakening) hallucinations.
Narcolepsy is caused by a deficiency in hypocretin (orexin). Hypocretin levels can be immunoassayed with a CSF sample. The pathophysiology of hypocretin neuronal loss is thought to be autoimmune, as 99% of affected individuals have a particular HLA-DQB1 allele.
Hypocretin-secreting neurons are located in the hypothalamus.
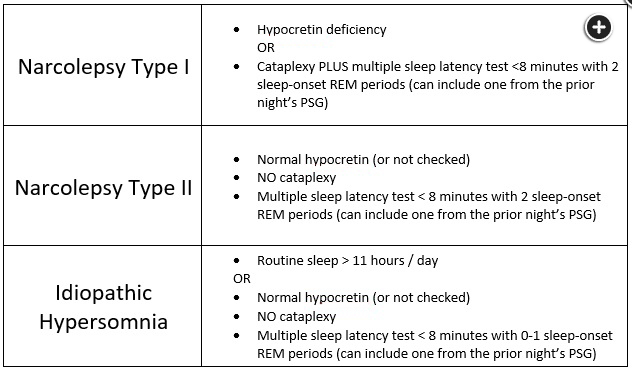
Narcolepsy type 1, narcolepsy type 2, and idiopathic hypersomnia all have formal diagnostic criteria. All three disorders require symptoms of sleepiness lasting at least 3 months. The diagnosis of narcolepsy type 1 also requires either hypocretin deficiency or a combination of cataplexy and a mean sleep latency of less than 8 minutes with two or more sleep-onset REM periods (which can include both MSLT naps and the preceding night’s PSG). Narcolepsy type 2 diagnosis requires a similarly abnormal MSLT, but without cataplexy, a low hypocretin level, or an alternate explanation for sleepiness. For a diagnosis of idiopathic hypersomnia, a patient must not have cataplexy or an alternate explanation for sleepiness, but must have either a mean sleep latency ≤8 minutes without two sleep-onset REM periods, or objectively confirmed total sleep times of more than 11 hours in a given day. These criteria are summarized in Figure 3. Again, all of these diagnoses require exclusion of alternate explanations for sleepiness.
Treatment
- treatment target:
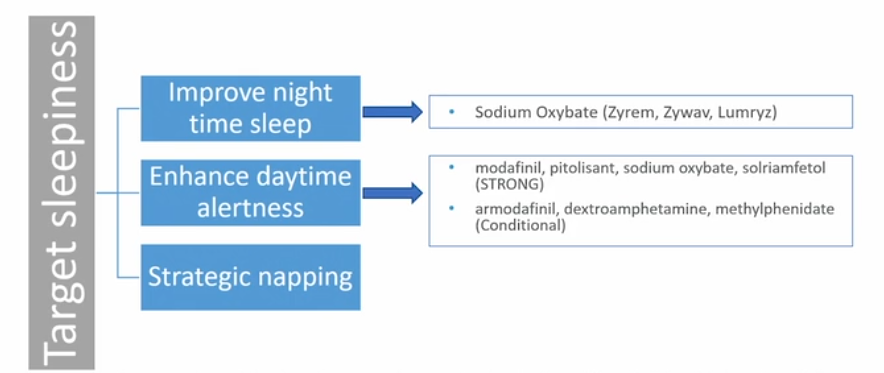
 - goal: reduced excessive day time sleepiness
- goal: reduced excessive day time sleepiness
- modafinil: novel stimulant, less addictive, first line
- older stimulants: methylphenidate, amphetamines
- effective but addictive
- bad side effects
- nonpharmacologic:
- taking scheduled naps
- good sleep hygiene
Treating cataplexy:
- sudden onset of muscle weakness
- triggers: intense emotional episodes (eg, anger, laughing, surprise)
- occurs in roughly 70% of patients with narcolepsy.
- Treatment: stimulants, nonpharmacologic
- can be treated with a serotonin-norepinephrine reuptake inhibitor (eg, venlafaxine) or selective serotonin reuptake inhibitor, and a tricyclic antidepressant can also be considered.
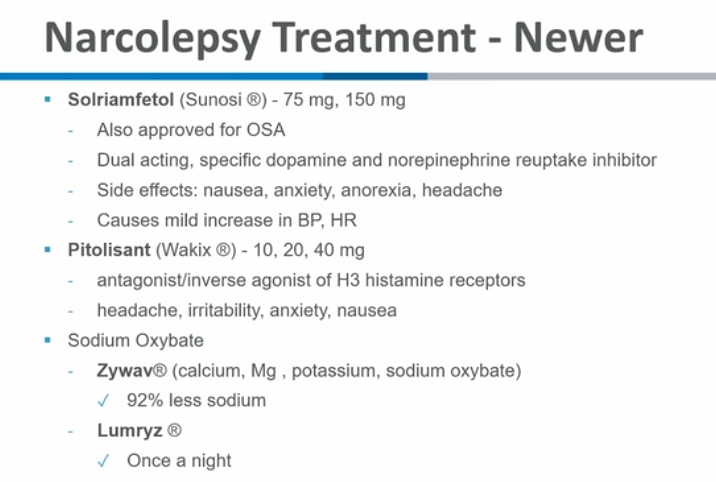
- Sodium oxybate (the salt form of gamma-hydroxybutyrate) can improve nocturnal sleep, relieve excessive daytime sleepiness and has anti-cataplectic properties; however, it is rarely used due to abuse potential and restrictive regulations.