PAD
- related: Cardiology and Hemodynamics
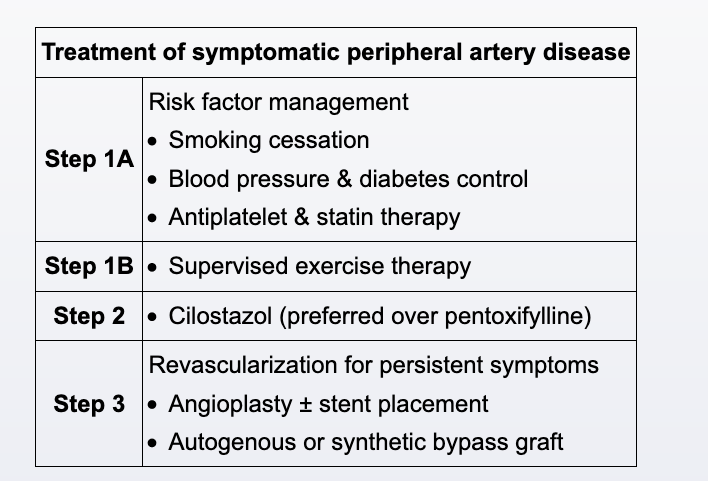
- manage risks: e.g. smoking cessation
- initial management: supervised exercise program best for claudication
- 30-45 minutes of supervised walking >3 times a week for >3 months
- Once the walking time required to develop claudication is determined, the sessions are gradually increased until the patient can walk for a longer period without developing symptoms.
- Patients may experience moderate increases in symptom-free walking distance.
- Pharm: antiplatelet and statin
- twice daily cilostazol can help with symptoms
- revascularization via stent or bypass reserved for critical limb ischemia
Limb Ischemia
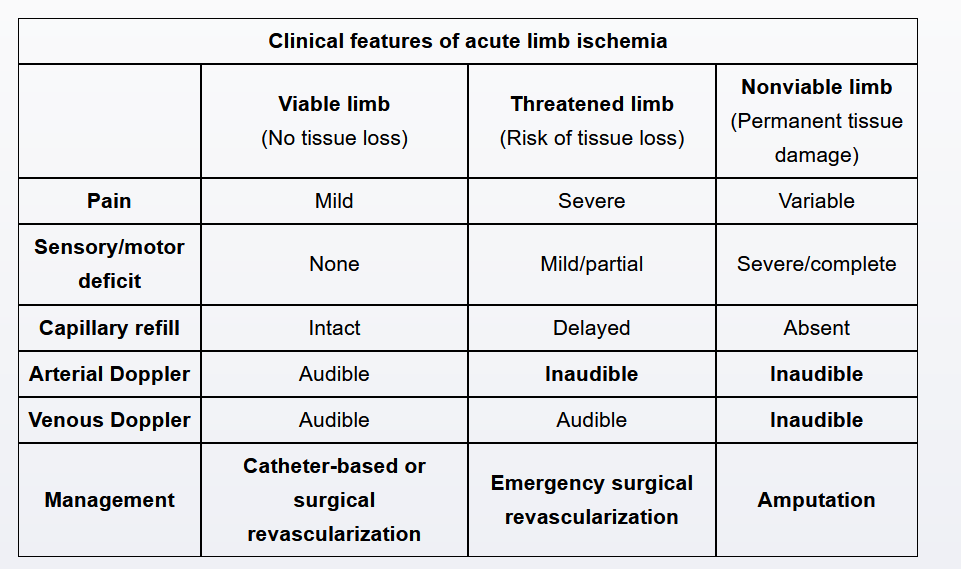
- acute limb ischemia (ALI)
- pathogenesis: sudden decrease in limb perfusion, often caused by acute arterial occlusion due to systemic embolism from a cardiac source (eg, atrial fibrillation, left ventricular thrombus, or septic emboli from infective endocarditis).
- sx: six P’s of acute ischemia: pain, pallor, paresthesia, pulselessness, poikilothermia, and paralysis.
- severe resting pain with sensory/motor loss
- delayed capillary refill
- no doppler signals
- imaging: CT angiography, duplex US, MRA for patients with viable ALI
- rx:
- anticoagulation, IV heparin bolus with infusion
- emergent surgical revascularization or catheter based thrombolytics