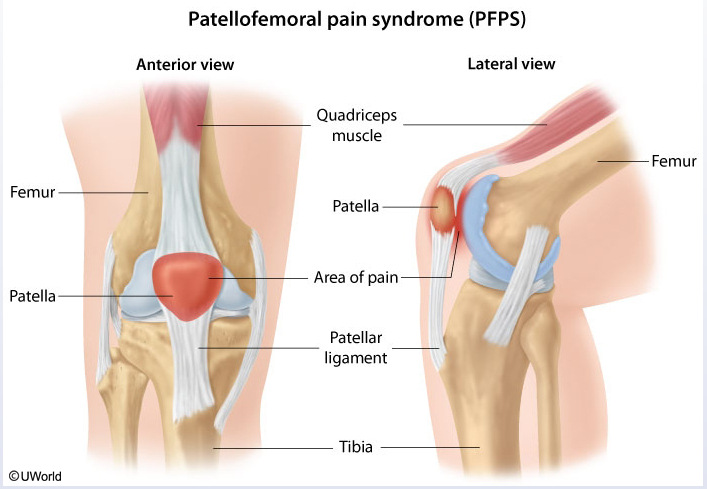
patellofemoral pain
- Patient population: common cause of knee pain in young athletes and predominantly affects women.
- Pathogenesis: chronic overuse or malalignment (eg, angular deformities, weakness of hip abductors) but can also be seen acutely following trauma.
- Sx:
- aching sensation and worsened by activities such as squatting or climbing stairs. Also can be worse with prolonged sitting due to sustained flexion.
- Although the anterior knee may have swelling, true knee effusions and hemarthrosis are not seen.
- Dx: clinical
- patellofemoral compression test (reproduction of pain when the quadriceps is contracted while the patella is compressed into the trochlear groove) is often helpful, but no single finding has high sensitivity or specificity.
- may also have crepitus with motion of the patella.
- Rx: reduce exercise intensity, nsaids, stretches

A 21-year-old student comes to the university health clinic due to left knee pain. For the last 3 weeks, she has had aching, poorly localized anterior knee pain that is worse when standing up from a low chair or when sitting in class for extended periods. The patient plays on a club softball team but is unable to play through a complete game due to the pain. Her medical history is unremarkable, and her only medication is an oral contraceptive. She does not use tobacco, alcohol, or illicit drugs. Temperature is 36.9 C (98.4 F), blood pressure is 118/70 mm Hg, and pulse is 68/min. BMI is 17 kg/m2. Inspection of the knee and leg is normal with no erythema, swelling, or obvious deformity. Active and passive range of motion is normal. Quadriceps strength is normal and symmetric, but squatting reproduces the pain. No focal tenderness is noted on palpation of the knee. Which of the following should be recommended to the patient at this time?
Links to this note
-
- Like patellofemoral pain syndrome, Osgood-Schlatter disease can cause anterior knee pain that is worse with squatting; however, it would not be seen in adult patients.