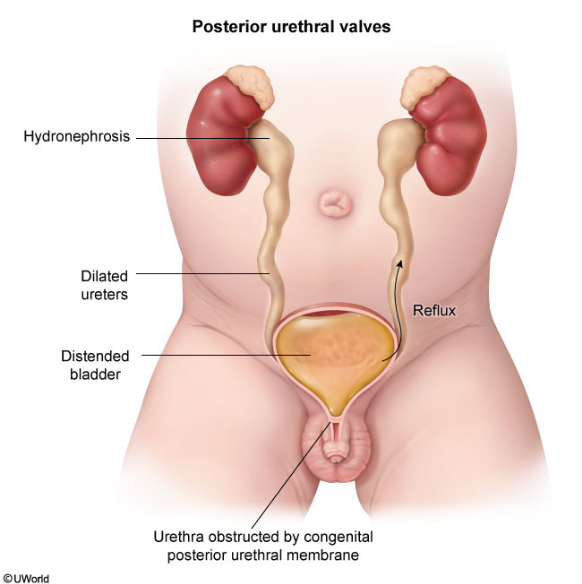
posterior urethral valve
- cause: congenital urethra obstruction by residual embryologic tissue during development in boys (most likely problem with wolffian duct insertion)
- sx: palpable bladder on exam, bilateral hydronephrosis, dilated/thickened bladder, oligohydramnios
- dx:
- antenatal ultrasound showing hydro, thickened/dilated bladder, dilated proximal urethra
- confirmed with voiding cystourethrogram (VCUG). VCUG is performed by catheterizing the patient, injecting radiopaque dye, and obtaining images during voiding. Infants with a PUV who undergo VCUG generally have dilated bladders, and approximately 25%-50% have some degree of vesicoureteral reflux and ureteral dilation due to the severe outflow obstruction caused by the PUV. However, the diagnosis is confirmed by visualization of a dilated proximal urethra when the catheter is removed (the catheter keeps the valve open and must be removed before the end of imaging).
- rx: Foley catheter placed to temporarily relieve the obstruction. When the infant’s condition is stabilized, cystoscopy allows direct visualization and ablation of the valve, which is curative.
Links to this note