Strongyloidiasis
- related: Infectious Disease
This patient from the Dominican Republic has a raised, erythematous, linear rash with significant eosinophilia, raising suspicion for strongyloidiasis.
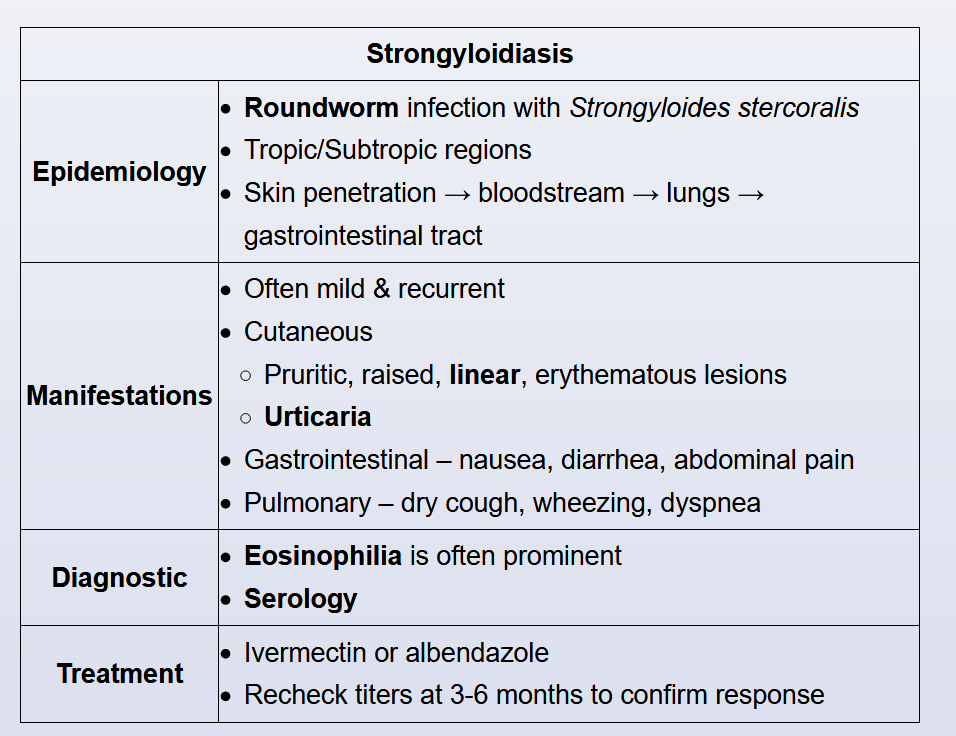
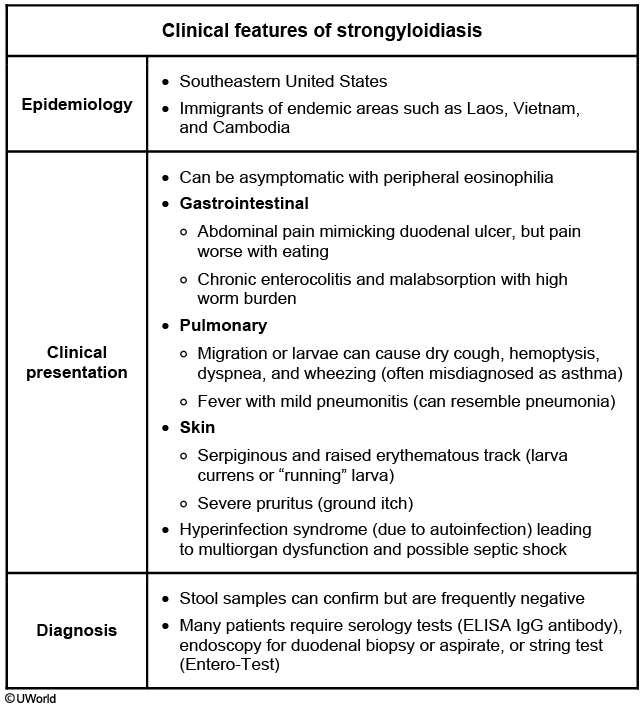
Strongyloidiasis is caused by Strongyloides stercoralis, a roundworm endemic to tropical and subtropical regions where prevalence can approach 25%. Inoculation occurs when human skin contacts filariform larvae in soil contaminated by human feces (from an infected host). After cutaneous penetration, the larvae migrate hematogenously to the lung where they enter the alveoli, ascend the tracheobronchial tree, and are swallowed. This results in chronic infection of the duodenum and jejunum with periodic autoinoculation through the perianal skin.
Symptoms reflect the worm lifecycle, and patients often have mild manifestations that wax and wane for years. Cutaneous findings include urticarial skin reactions and periodic erythematous, raised tracks on the buttocks or thighs (secondary to autoinoculation); gastrointestinal (eg, nausea, diarrhea, pain) and pulmonary (eg, dry cough, wheezing) symptoms may also occur. Laboratory results usually show prominent eosinophilia.
Stool examination has low sensitivity (<50%) for diagnosis due to periodic shedding of organisms; diagnosis is typically confirmed with serology. Treatment with ivermectin or albendazole is usually curative, but repeat serologies should be performed at 3-6 months as treatment failures can occur.