TTP symptoms, diagnosis, scoring
- related: TTP thrombotic thrombocytopic purpura
- tags: #literature #hemeonc
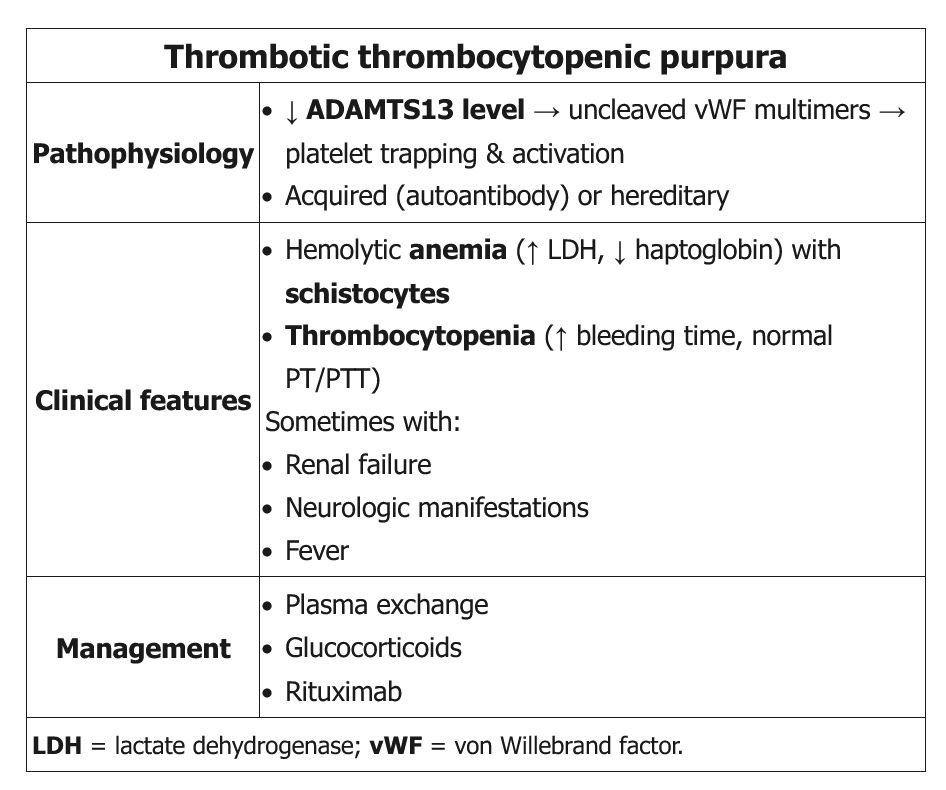
The diagnosis of TTP should be considered in a previously healthy patient presenting with MAHA and thrombocytopenia without another clear cause.
The pentad classically taught of MAHA, thrombocytopenia, fever, and neurologic and renal dysfunction is not always present. Although neurologic findings are fairly common, clinically significant renal disease is rare, although mild renal disease is often found. The diagnosis of TTP is confirmed when reduced ADAMTS13 activity is documented.
- neurologic sx, rash, AKI, chest pain, abdominal pain
- normal coagulation studies such as DIC panel
- negative Coombs test
- smear: schistocytes
- ADAMTS13 < 10%
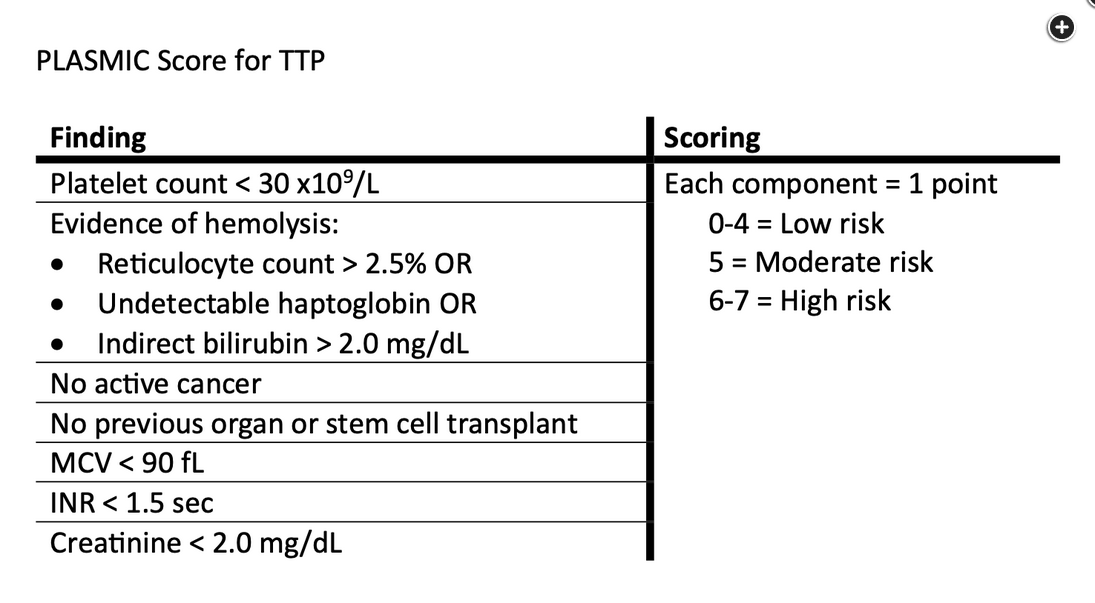
While awaiting confirmatory testing, there is an assessment score that can be used called the PLASMIC score (Figure 4).
Links to this note
Footnotes
-
Paydary K, Banwell E, Tong J, et al. Diagnostic accuracy of the PLASMIC score in patients with suspected thrombotic thrombocytopenic purpura: a systematic review and meta-analysis. Transfusion. 2020;60(9):2047-2057. PubMed ↩
-
Zheng XL, Vesely SK, Cataland SR, et al. ISTH guidelines for the diagnosis of thrombotic thrombocytopenic purpura. J Thromb Haemost. 2020;18(10):2486-2495. PubMed ↩