acute eosinophilic pneumonia diagnosis include eosinophils on BAL, pulmonary infiltrate, febrile illness
- related: acute and chronic eosinophilic pneumonia AEP and CEP
- tags: #permanent
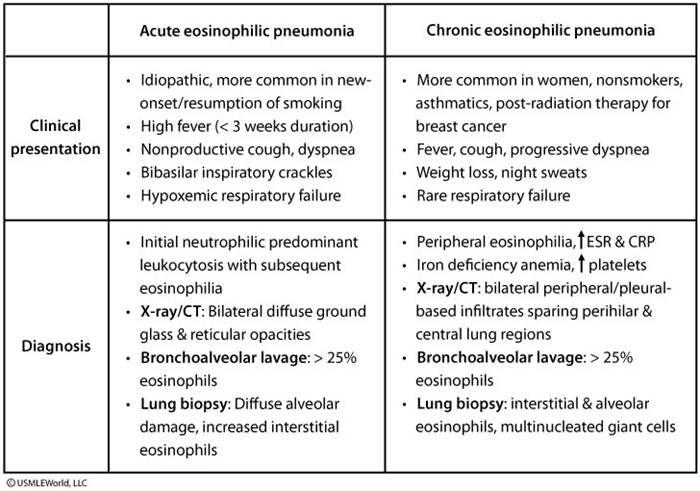
- acute to subacute febrile illness
- hypoxemic respiratory failure
- diffuse pulmonary opacities
- BAL showing >25% eosinophils (eosinophilic BAL points to atypical infections and atopic conditions, pulmonary eosinophilia differential diagnosis). 1
- clinically, pulmonary infiltrates on chest imaging with peripheral eosinophilia over 1500 can be used as diagnosis 2