AKI note 2 24
- related: Nephrology
Definition
- KDIGO criteria

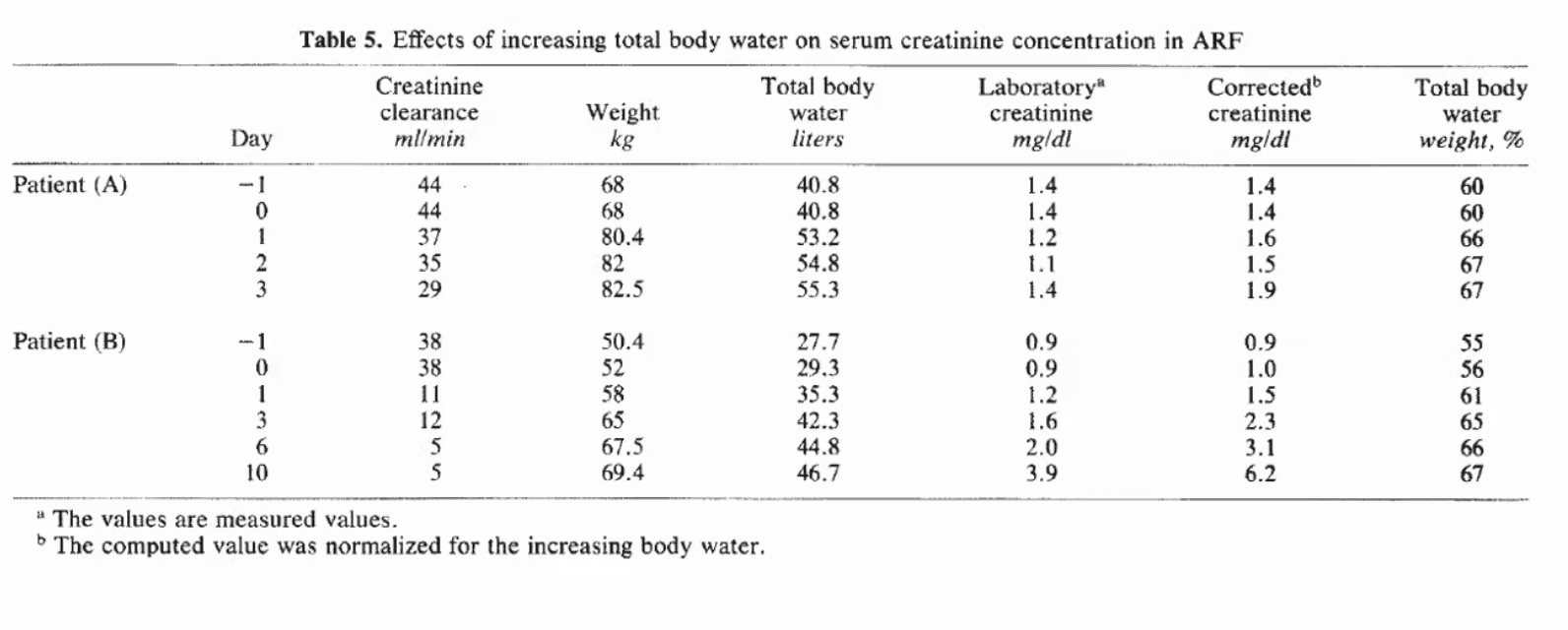
- creatinine can be affected by medication, secretion, muscle mass
- generation of creatinine lower in septic states
- volume resuscitation can dull change in GFR
Causes
- Sepsis: most common cause in ICU
- cardiac surgery: 2nd most common cause
- acute liver failure, acetaminophen toxicity
- intra-abdominal HTN: decreased perfusion
- hepatorenal syndrome
- malignancy
- cardiorenal syndrome
Indications for dialysis
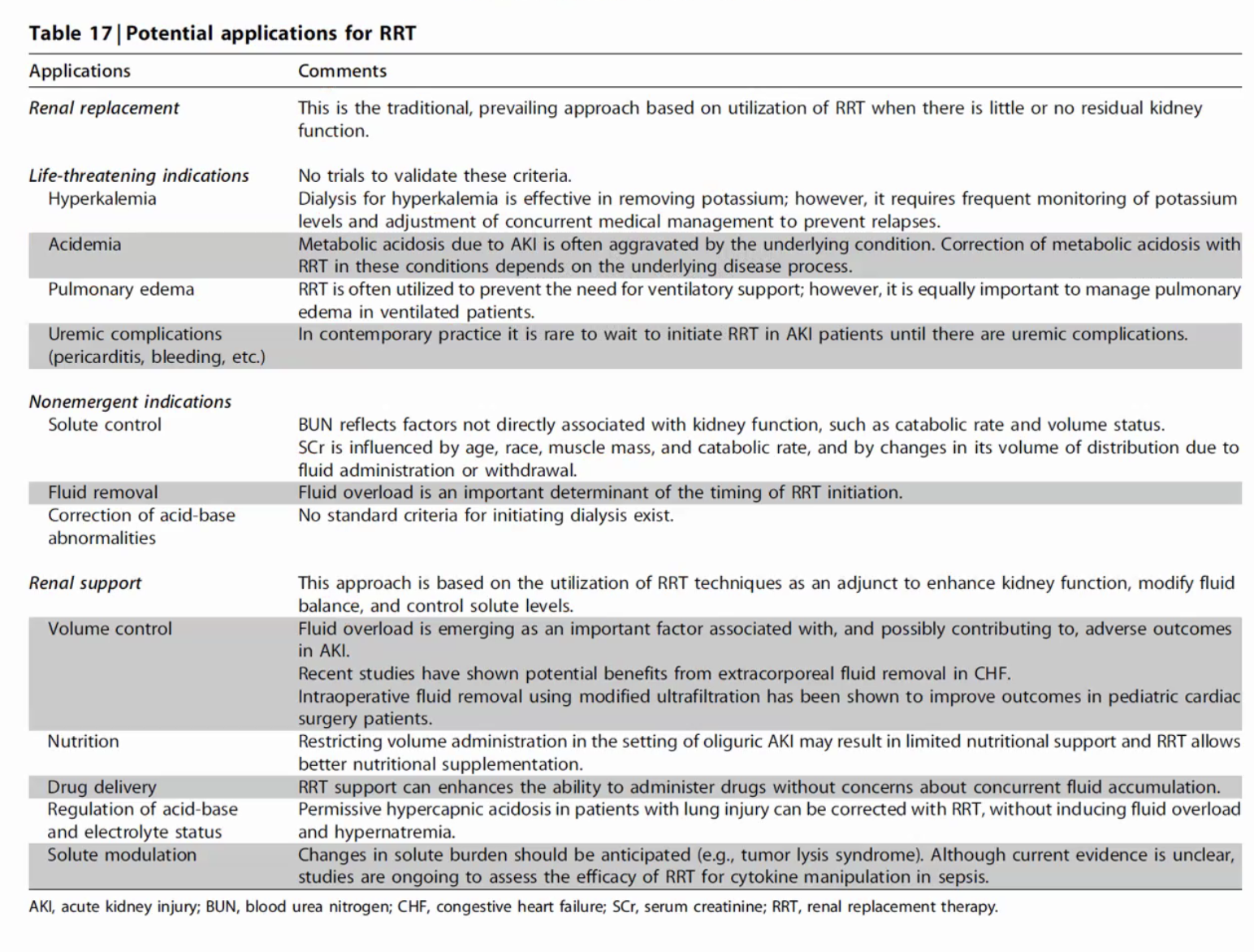
- urea > 150
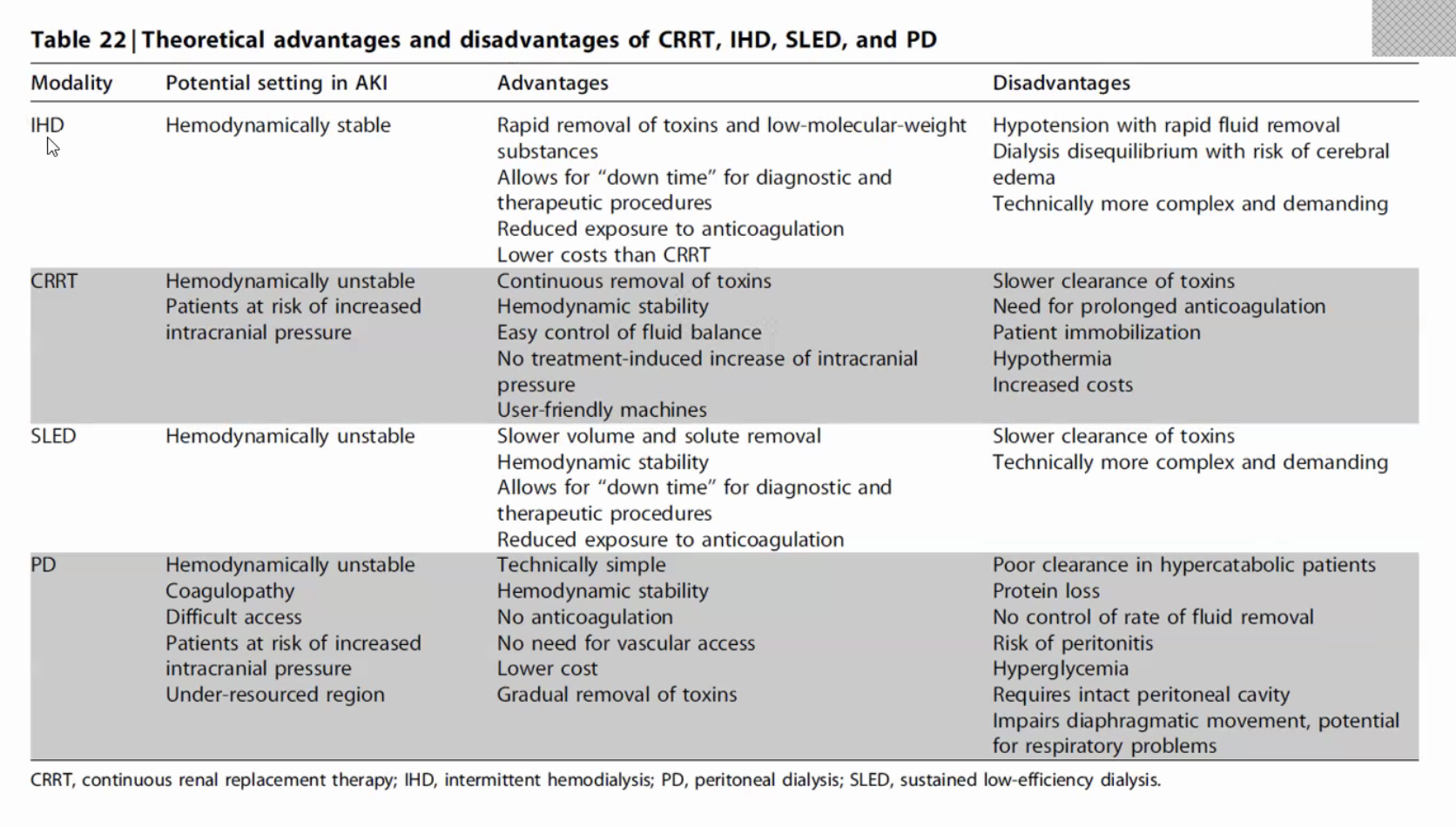
- iHD: mostly does not require heparin during iHD inpatient unless at risk of clotting
- outpatient: IV heparin during dialysis due to micro clots
- dialysis disequilibrium syndrome: urea removal too quickly
- CRRT: not good for ingestions because slower
- hybrid treatment
- SLED: intermittent HD 6 hour treatment. Slower iHD
- prolonged intermittent renal replacement therapy: a longer dialysis 8-12 hours treatment
- PD can be acute by surgically place PD catheter
Hyponatremia
- is it dangerous: give 3% Na
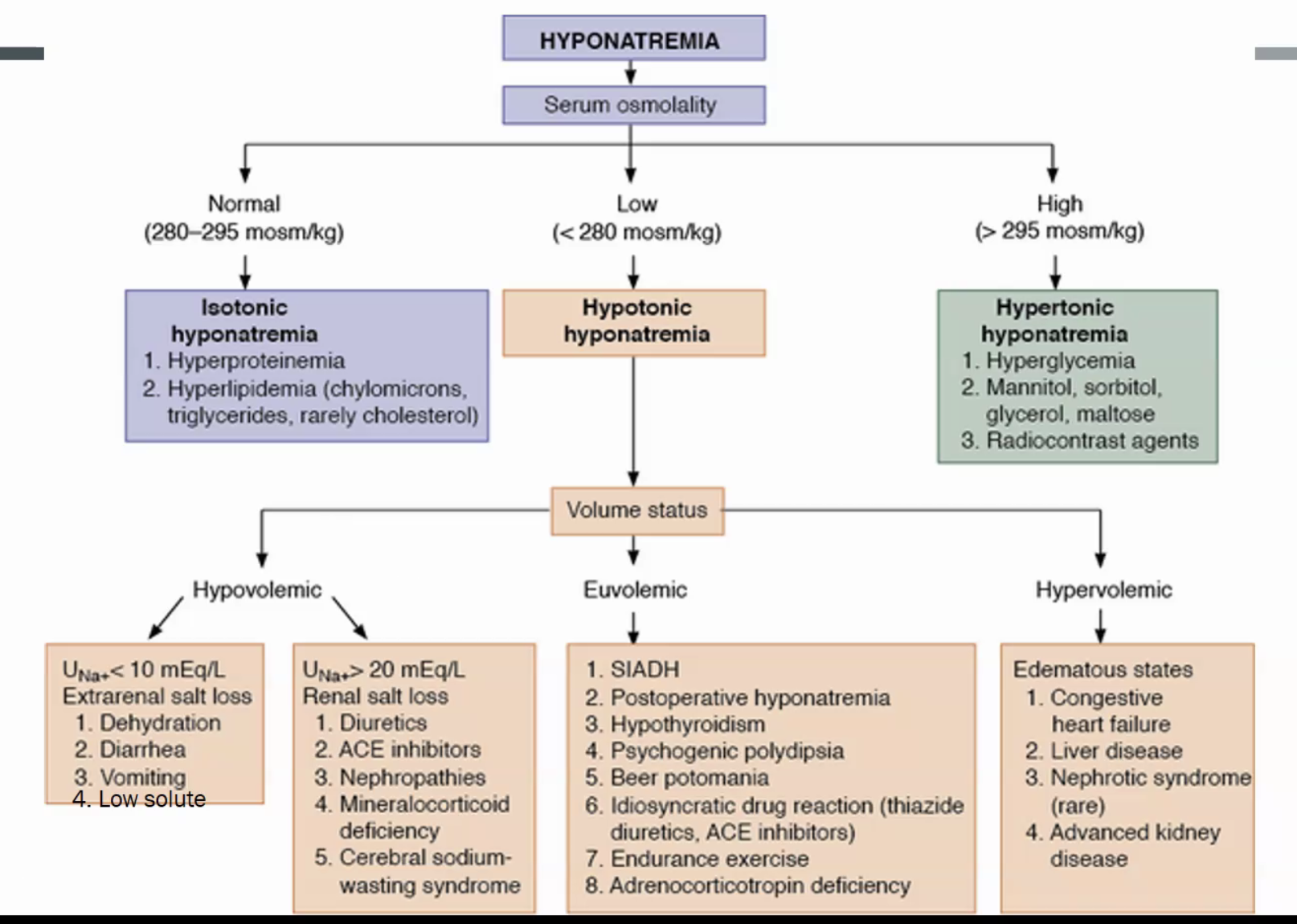
- know if it’s true hyponatremia (serum osm)
- hypo-osmolar: true
- isoosmolar: interfering substance such as TG, IVIG, protein. Check whole blood Na
- hyper-osmolar (osm > 310): mannitol, hyperglycemia
- decide volume status
SIADH
- rule out hypothyroidism, adrenal insufficiency
- causes:
- uncontrolled pain, nausea
- SSRI, AED’s, anti neoplastics
- ecstasy: increase ADH secretion
- SCC
- COPD
- diuretics (thiazides)
- diagnosis: low serum Na, high urine Na, high urine osm
- treatment: fluid restriction
- 1L very little fluid
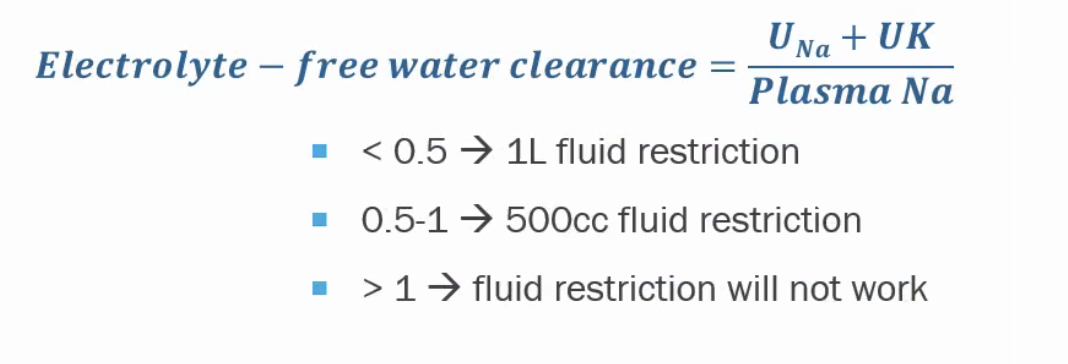
- how much urine is water vs electrolytes
- 3% if severe or pt NPO
- salt tabs
- Ure-Na, palatable urea: makes BUN go up and kidney have osmotic diuresis
Osmotic demylelination syndrome
- over correct Na
- quadriplegia, mentation changes, dysphagia/dysarthria
- diagnose with MRI
- correction: 6-10 mEq/day is ok, more 6
- potassium repletion contributes to increase in Na
- pt very dehydrated will have high ADH and will self correct when ADH stimulus shut off, easy to over correct (when urine output starts to go up)
- If over correction: re under correct
- DDAVP (1-2 mcg subq/IV q8h)
- D5
- vaptans
- sometimes give DDAVP/3% together
Hypernatremia
- most common cause is pt not able to communicate free water loss
- vent/trach: high insensible loss
- hyperglycemia: (glucose - 100) x 1.6 + measured Na
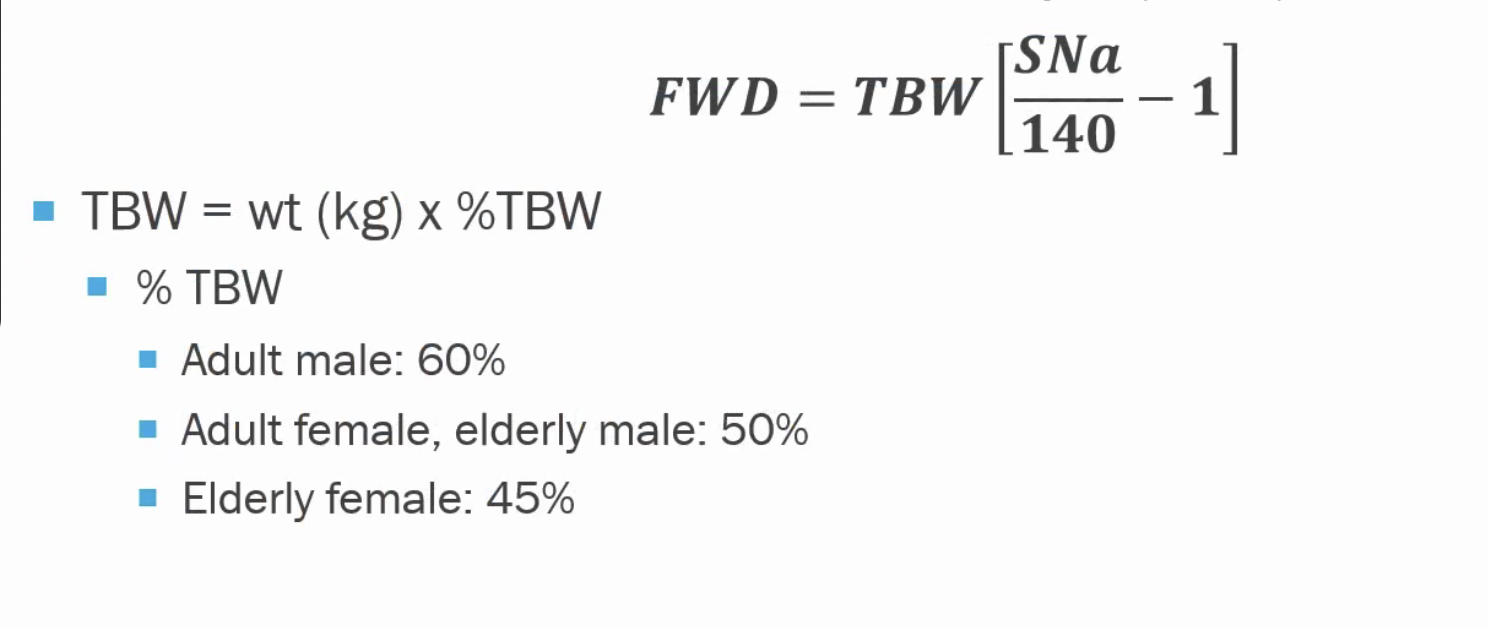
- correction: replace free water + urinary loss + insensible loss
DI
- central, nephrogenic
- drug induced (lithium)
- gestational (degrade vasopressin by vasopressinase by placenta)
- diagnosis
-
4L output per day
- low urine osm, ± hypernatremia
- water deprivation test
- complete: doesn’t change urine osm
- partial: changes some
- trial of DDAVP
-