APRV autopeep problem
- related: APRV ventilation
- tags: #literature #icu
An underappreciated aspect of APRV is that the short expiratory time often recommended by those experienced with using APRV results in the buildup of significant auto-PEEP. In this patient, auto-PEEP should be expected, since the expiratory flow does not return to zero during the short expiratory time (Figure 2, yellow arrow).
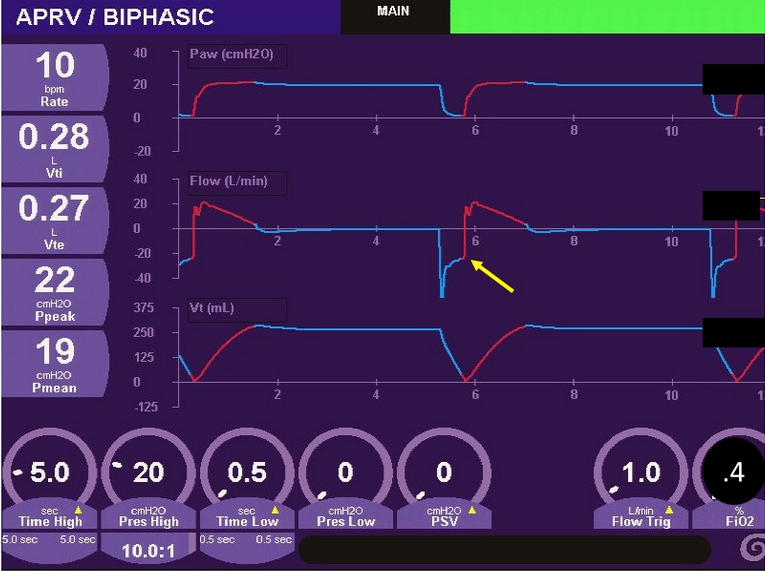
- Airway pressure, flow, and volume over time from a patient on APRV. Yellow arrow indicates incomplete exhalation suggesting the presence of auto-PEEP.
Indeed, an expiratory pause maneuver demonstrates a total of 12.8 cm H2O auto-PEEP above the set PEEP of 0 cm H2O (Figure 3, yellow arrow).
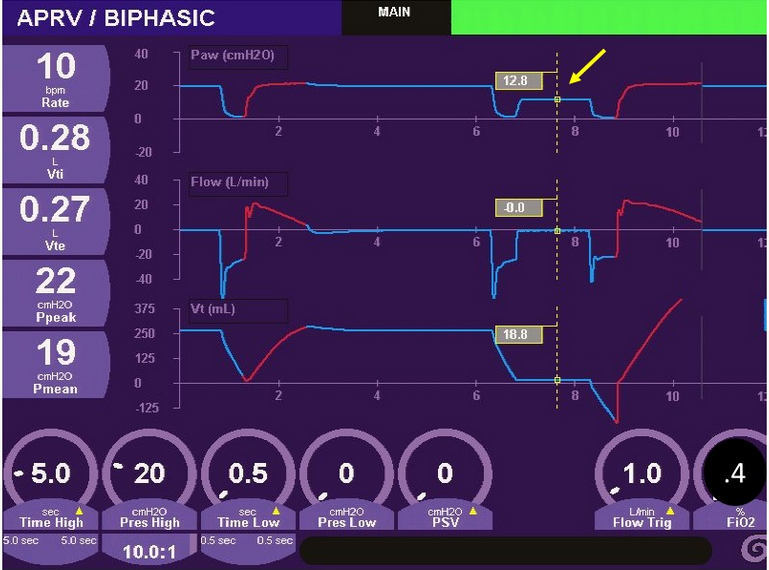
- Airway pressure, flow, and volume over time from a patient receiving APRV. Yellow arrow indicates a measured auto-PEEP of 12.8 cm H2O obtained from an expiratory pause maneuver.
At the same time, the set Phigh of 20 cm H2O is identical to the end-inspiratory Pplat in the lungs. Importantly, the calculated driving pressure (Pplat − PEEP) using the applied PEEP (0 cm H2O) yields an excessive value of 20 cm H2O. However, when using the correct PEEP level, driving pressure is in a relatively safe range (ie, 20 − 12.8 = 7.2 cm H2O).
It is important to remember that auto-PEEP and applied PEEP distribute differently and may have different recruitment effects. Applied PEEP distributes equally throughout the lungs to all units with patent airways. In contrast, auto-PEEP develops predominantly in units with slow expiratory time constants (ie, high-resistance, high-compliance units) that may not be optimal in parenchymal lung injury.
AutoPEEP can be particularly problematic if the patient has underlying airflow obstruction, and it can result in dynamic hyperinflation and barotrauma. In a prospective study comparing multiple Tlow levels, researchers found that Tlow of 0.5 s was accompanied by lower tidal volumes, increased autoPEEP, and rising PaCO2 compared with longer Tlows studied. The spontaneous breaths that are permitted throughout the breath cycle can improve ventilation of dependent lung units, increase venous return and cardiac output, and reduce sedation requirements. However, vigorous inspiration can raise transpulmonary pressure, and spontaneous breaths taken while lungs are inflated (during Phigh) can produce excessive tidal volumes (Figure 2, arrow), both of which situations are potentially injurious to the lungs.
Links to this note
Footnotes
-
Chen C, Zhen J, Gong S, Yan J, Li L. Efficacy of airway pressure release ventilation for acute respiratory distress syndrome: a systematic review with meta-analysis. Ann Palliat Med. 2021;10(10):10349-10359. PubMed ↩
-
Lalgudi Ganesan S, Jayashree M, Chandra Singhi S, Bansal A. Airway pressure release ventilation in pediatric acute respiratory distress syndrome: a randomized controlled trial. Am J Respir Crit Care Med. 2018;198(9):1199-1207. PubMed ↩
-
Neumann P, Golisch W, Strohmeyer A, Buscher H, Burchardi H, Sydow M. Influence of different release times on spontaneous breathing pattern during airway pressure release ventilation. Intensive Care Med. 2002;28(12):1742-1749. PubMed ↩
-
Othman F, Alsagami N, Alharbi R, Almuammer Y, Alshahrani S, Ismaeil T. The efficacy of airway pressure release ventilation in acute respiratory distress syndrome adult patients: a meta-analysis of clinical trials. Ann Thorac Med. 2021;16(3):245-252. PubMed ↩
-
Rose L, Hawkins M. Airway pressure release ventilation and biphasic positive airway pressure: a systematic review of definitional criteria. Intensive Care Med. 2008;34(10):1766-1773. PubMed ↩
-
Zhou Y, Jin X, Lv Y, et al. Early application of airway pressure release ventilation may reduce the duration of mechanical ventilation in acute respiratory distress syndrome. Intensive Care Med. 2017;43(11):1648-1659. PubMed ↩