APRV settings
- related: understanding of ventilators
- tags: #literature #pulmonology #icu
APRV is a mode that is based on machine/patient-triggered, pressure-targeted, and time-cycled breaths that is set in a prolonged inspiratory time/short expiratory time configuration (inverse ratio ventilation). It is similar in concept to older inverse ratio strategies but differs in that spontaneous breaths are allowed. In theory, inverse ratio strategies offer the advantage of mean airway pressure elevations and consequent alveolar recruitment without having to add PEEP or tidal volume. Outcome studies, however, are limited and conflicting.
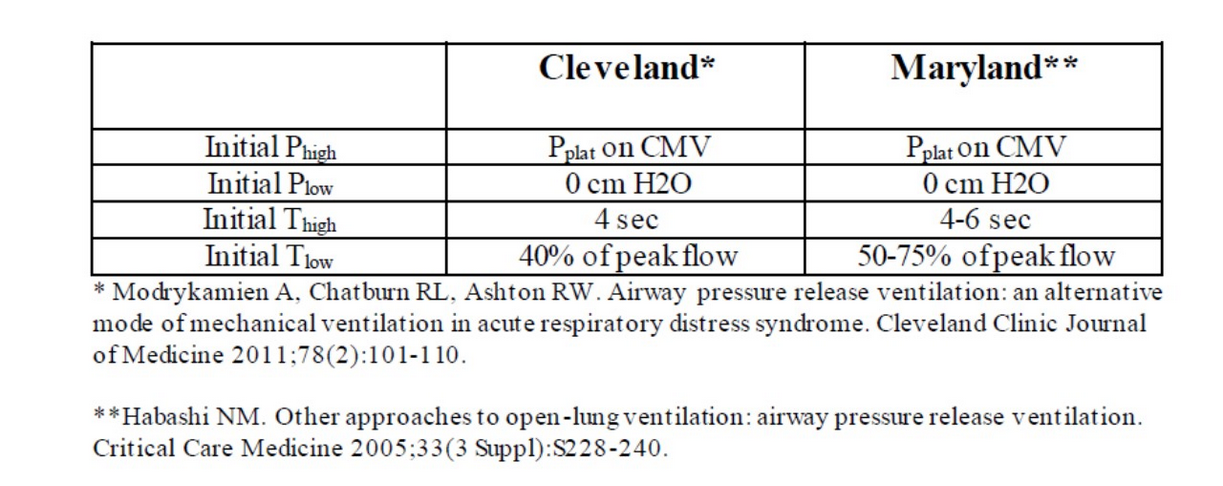
Consensus about proper APRV settings does not exist. Figure 4 summarizes recommendations from two groups with considerable APRV experience. An additional feature to APRV that clinicians need to appreciate is that spontaneous breaths, with or without pressure support, are allowed (even encouraged) during the inflation from Phigh. When these are present (not in this patient), the patient-generated negative pressure can add to the Phigh to increase end-inspiratory transpulmonary pressure to potentially dangerous levels.
Biphasic ventilation (also called bi-vent, bilevel, or biphasic) is a mode of ventilation in which continuous positive airway pressure is cycled between high pressure (Phigh) and low pressure (Plow or PEEP). Mandatory breaths are pressure limited and time cycled. Airway pressure release ventilation (APRV) is a unique form of biphasic ventilation characterized by very long inspiratory time and very brief expiratory time to low set PEEP during which time the breath is “released” (Figure 1). A key feature of both biphasic ventilation and APRV is that spontaneous breaths are permitted to occur throughout the breath cycle (Figure 2, arrow) regardless of whether the lungs are inflated with a positive pressure breath (Phigh) or not (Plow or PEEP).
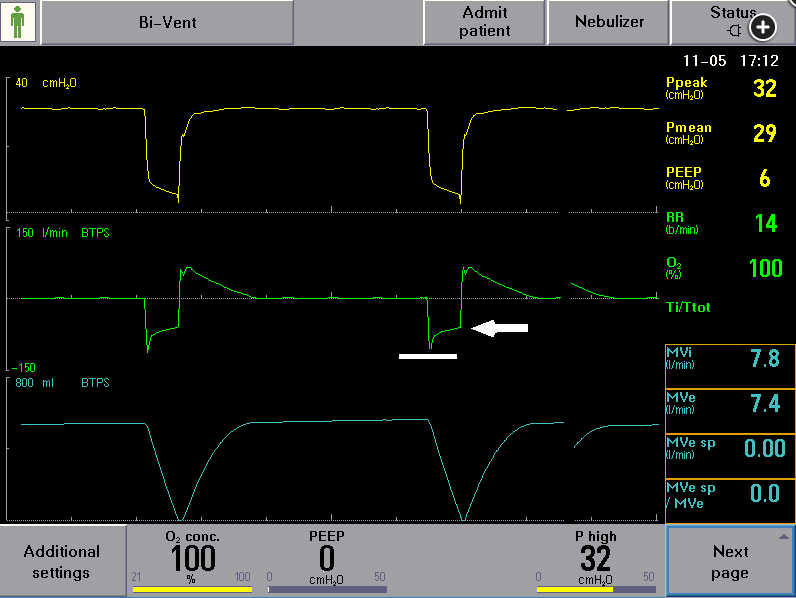
APRV. Line denotes peak expiratory flow; arrow corresponds to expiratory flow of about 50% of peak expiratory flow at time of transition to breath delivery.
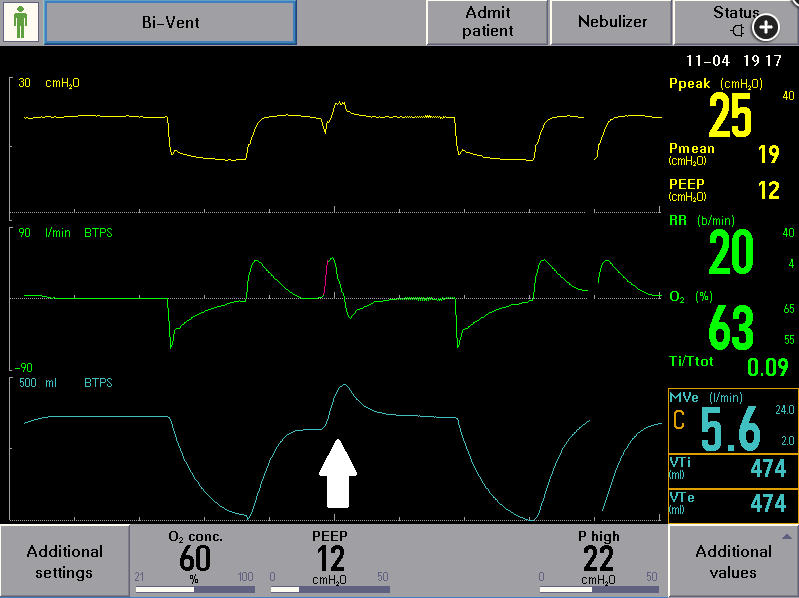
Bi-vent ventilation. Note spontaneous breath (arrow) while lungs are inflated.
As seen in Figure 1, APRV typically is set to have a very long high pressure time (Thigh)—often 80% to 90% of the breath cycle and a very brief low pressure time (Tlow or PEEP)—often 0.4 to 0.8 s (Figure 1) to PEEP of 0 to 5 cm H2O.
APRV users often adjust the duration of Tlow by transitioning to Phigh when the expiratory flow has decreased to about 50% (Figure 1, arrow) of the peak expiratory flow (Figure 1, line). Peak inspiratory flow is not considered in this process.1234567
Links to this note
Footnotes
-
Chen C, Zhen J, Gong S, Yan J, Li L. Efficacy of airway pressure release ventilation for acute respiratory distress syndrome: a systematic review with meta-analysis. Ann Palliat Med. 2021;10(10):10349-10359. PubMed ↩
-
Lalgudi Ganesan S, Jayashree M, Chandra Singhi S, Bansal A. Airway pressure release ventilation in pediatric acute respiratory distress syndrome: a randomized controlled trial. Am J Respir Crit Care Med. 2018;198(9):1199-1207. PubMed ↩
-
Neumann P, Golisch W, Strohmeyer A, Buscher H, Burchardi H, Sydow M. Influence of different release times on spontaneous breathing pattern during airway pressure release ventilation. Intensive Care Med. 2002;28(12):1742-1749. PubMed ↩
-
Othman F, Alsagami N, Alharbi R, Almuammer Y, Alshahrani S, Ismaeil T. The efficacy of airway pressure release ventilation in acute respiratory distress syndrome adult patients: a meta-analysis of clinical trials. Ann Thorac Med. 2021;16(3):245-252. PubMed ↩
-
Rose L, Hawkins M. Airway pressure release ventilation and biphasic positive airway pressure: a systematic review of definitional criteria. Intensive Care Med. 2008;34(10):1766-1773. PubMed ↩
-
Zhou Y, Jin X, Lv Y, et al. Early application of airway pressure release ventilation may reduce the duration of mechanical ventilation in acute respiratory distress syndrome. Intensive Care Med. 2017;43(11):1648-1659. PubMed>) ↩