calculating driving pressure in pressure support mode
- related: understanding of ventilators
- tags: #literature #pulmonology
 Pressure, flow, and volume over time from a patient breathing spontaneously on pressure-support ventilation. Setting an intermittent mandatory ventilation rate of 1 allows for delivery of a control breath with a comparable volume and an inspiratory pause from which a measurement of a plateau pressure can be made (arrow).1
Pressure, flow, and volume over time from a patient breathing spontaneously on pressure-support ventilation. Setting an intermittent mandatory ventilation rate of 1 allows for delivery of a control breath with a comparable volume and an inspiratory pause from which a measurement of a plateau pressure can be made (arrow).1
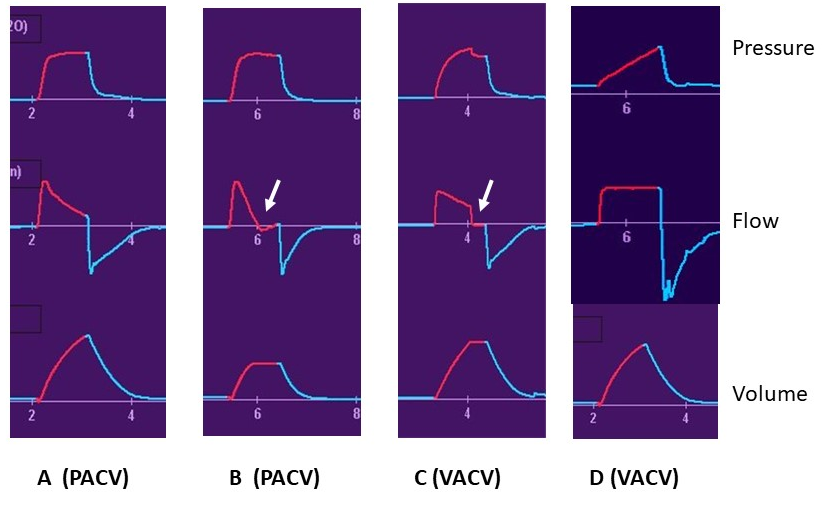
Pressure, flow, and volume graphics over time during four passive breaths. Arrows indicate short periods of zero flow enabling determinations of plateau airway pressure.
Plateau pressure measurements at end-inspiration (Pplat) are made under no-flow conditions and represent the alveolar distending pressure. No-flow conditions can be created at the end of a breath in any passive mode either by having a total inspiratory time longer than is required for set breath delivery or by manually holding the lung inflated after flow has ceased (the inspiratory hold or pause button on most modern ventilators, available in both volume and pressure-controlled modes). Breaths B and C both have such a pause in place (Figure 2, arrows) (choice B is correct); Breaths A and D do not (choices A, C, D incorrect). The end-inspiratory alveolar pressure (Pplat) can yield important information about lung mechanics and impact of ventilator settings. Assuming the pleural pressure is low (normal chest wall compliance), this alveolar pressure is a surrogate for transpulmonary pressure (TPP), the actual stretching pressure on alveolar structures. Not only can this be used to assess the maximal stretch (static stress and strain) on the lung, it can also be used to calculate the driving pressure (DP = Pplat − PEEP) required to tidally distend the lungs (dynamic stress and strain). There is growing interest in using DP as an aid in setting both tidal volume and PEEP. As noted, using Pplat as a surrogate for end-inspiratory TPP assumes a low pleural pressure on the other side of alveolar structures. This is a reasonable assumption in patients with near normal chest wall compliance. However, under circumstances where chest wall compliance is low (eg, abdominal compartment syndrome, surgical binders, obesity), this assumption is not valid and Pplat will overestimate actual TPP. This must be accounted for in assessing lung mechanics either empirically or with the use of pleural pressure sensors (eg, esophageal balloon pressures).2345
Links to this note
Footnotes
-
Brochard L, Martin GS, Blanch L, et al; Clinical review: Respiratory monitoring in the ICU - a consensus of 16. Crit Care. 2012;16(2):219. PubMed ↩
-
MacIntyre NR. Respiratory system mechanics. In: MacIntyre NR, Branson RD, eds. Mechanical Ventilation. 2nd ed. Philadelphia, PA: WB Saunders; 2008:159-170. ↩
-
Marini JJ, Rodriguez M, Lamb V. Bedside estimation of the inspiratory dynamics relevant to mechanical ventilation. Chest. 1986;89:56-62. ↩
-
Truwit JD, Marini JJ. Evaluation of thoracic mechanics in the ventilated patient. J Crit Care. 1988;3:133-150;192-213. ↩