combined pulmonary fibrosis emphysema CPFE
- related: ILD Interstitial Lung Disease or Diffuse Parenchymal Lung Disease
- tags: #literature
- patients with ILD can have emphysema thought to be from cigarette smoking
- emphysema is usually in upper lobe with bullae

- PFT finding in combined pulmonary fibrosis emphysema CPFE shows normal volume, reduced DLCO
- antifibrotics may or may not work: excluded from studies
- FVC progression for combined pulmonary fibrosis emphysema CPFE may be misleading
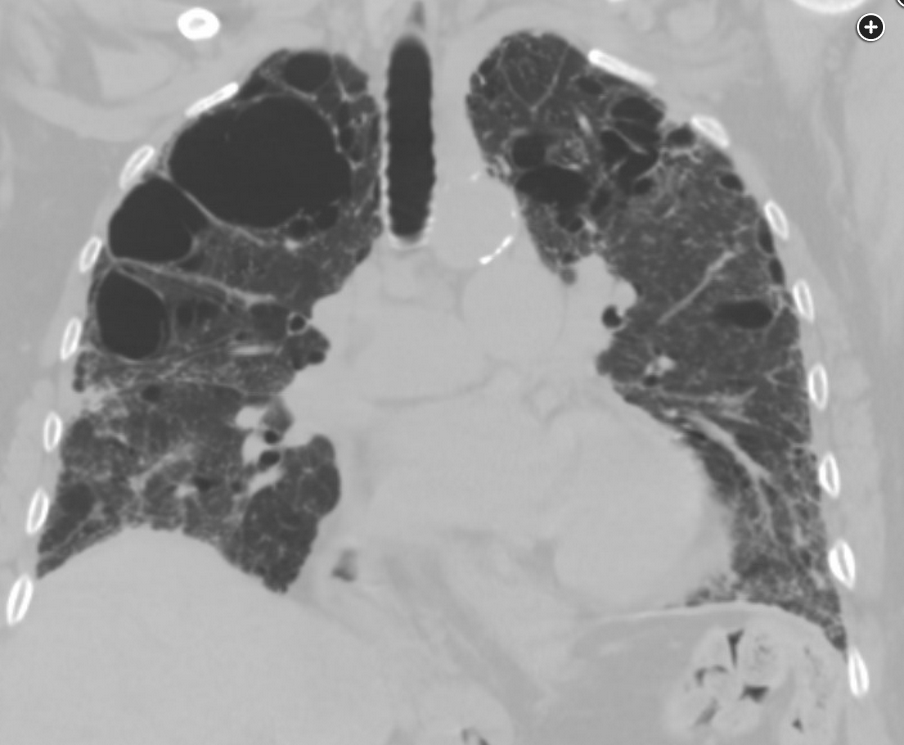
For the past 20 years, there has been an increasing appreciation for the entity most recently named the “syndrome of combined pulmonary fibrosis and emphysema” (CPFE). Patients with CPFE may have severe hypoxemia and dyspnea with relatively preserved spirometry and lung volumes owing to the countervailing influences of emphysema and pulmonary fibrosis in the lungs. Mean age at diagnosis is 65 to 70 years old, and there is a strong male predilection. The majority of patients have normal FEV1/FVC ratio. DLCO may be markedly reduced, and pulmonary hypertension is a common complication. It is uncertain whether this syndrome represents coexistence of two independent processes (emphysema and pulmonary fibrosis) that offset each other with respect to the physiology underlying pulmonary function testing (eg, low compliance with pulmonary fibrosis, high compliance with emphysema) or a single pathophysiology. Chest CT scan shows elements of both emphysema (particularly observed in the upper zones) and pulmonary fibrosis, at times with traction bronchiectasis and honeycombing (see Figure 2). Patients may present with acute exacerbations similar to those seen in patients with pulmonary fibrosis. There are no clear, evidence-based guidelines for treatment; however, antifibrotic agents have been used, and pulmonary hypertension, when present, is treated in usual ways.
Pulmonary hypertension has been reported in 15% to 55% of patients with CPFE. Lung cancer is another major complication in these patients, with adenocarcinoma and squamous cell carcinoma predominating. Although results vary among studies, total survival from lung cancer is poorer in this group of patients than in the general population of patients with carcinoma of the lung. The presence of honeycombing and inability to tolerate surgical resection may contribute to these worse outcomes.
Outcomes in patients with CPFE tend to be worse than in patients with emphysema alone. Data are variable when comparing survival in this group of patients when compared with those with pulmonary fibrosis alone. Decline in pulmonary function is slower in patients with CPFE than in patients with emphysema or pulmonary fibrosis alone. FVC is not a predictor of survival unless it is less than 50% of predicted; DLCO, however, does portend worse outcomes. Complications of CPFE, such as pulmonary hypertension and lung cancer, are associated with higher mortality. There are no data at this time to inform us about the utility of antifibrotics in this disease. Similarly, treatment of pulmonary hypertension pharmacologically is not well studied. Maintenance of SpO2 at or above 90% is recommended. Lung transplantation should be considered for appropriate patients, although data on its feasibility in these patients are limited.1
Links to this note
-
ILD Interstitial Lung Disease or Diffuse Parenchymal Lung Disease
-
FVC progression for combined pulmonary fibrosis emphysema CPFE may be misleading
-
PFT finding in combined pulmonary fibrosis emphysema CPFE shows normal volume, reduced DLCO