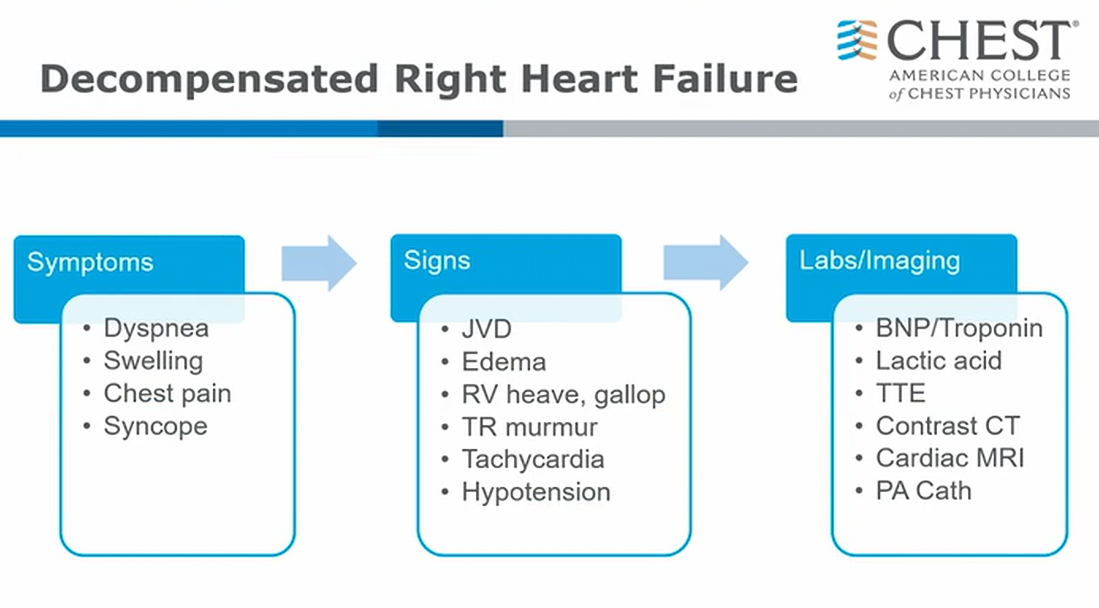
decompensated RV failure
Physiology
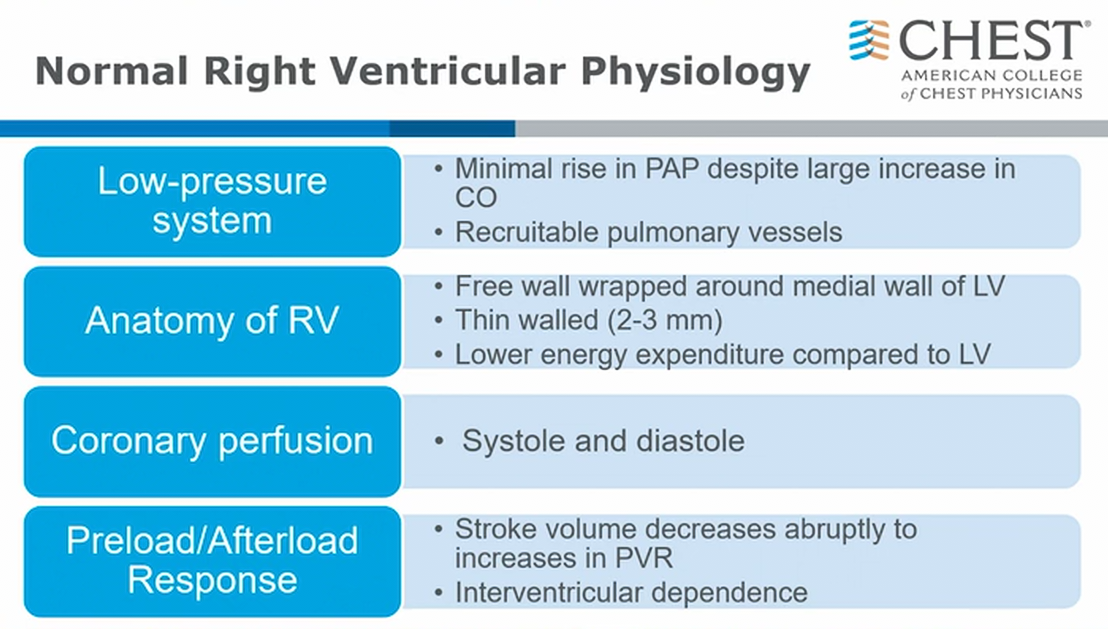
- RV is princess ventricle: very fragile
- usually low pressure system: 20 mmHg
- RV perfusion: systole and diastole via RCA
- changes in RV morphology can affect filling of LV
Diagnosis
Causes in ICU
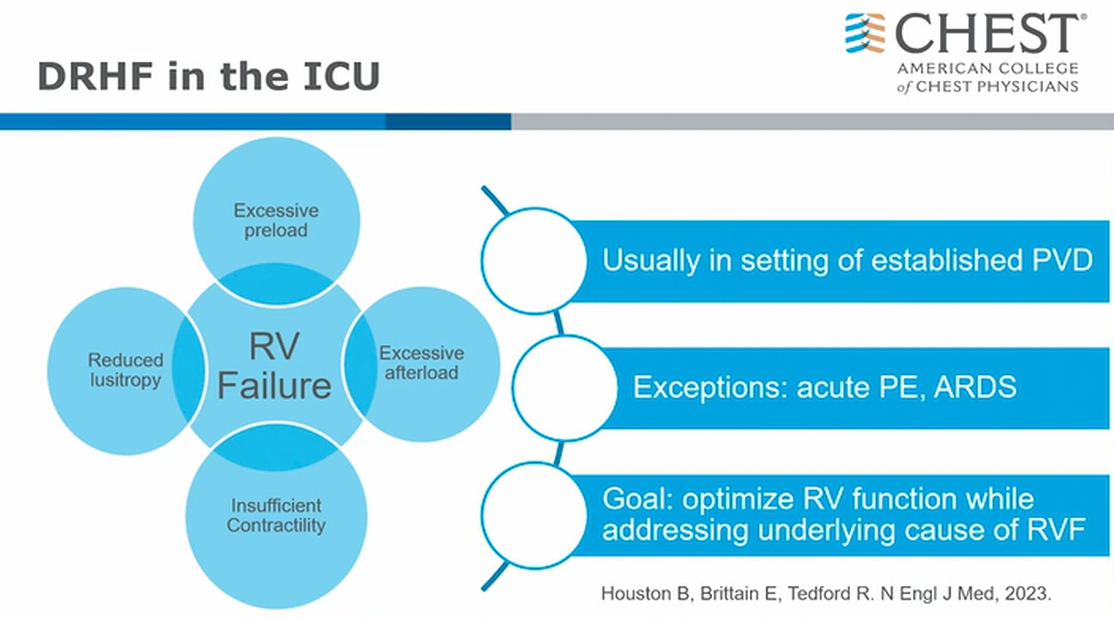
- RV failure causes
- reduced lusitropy: reduced relaxation
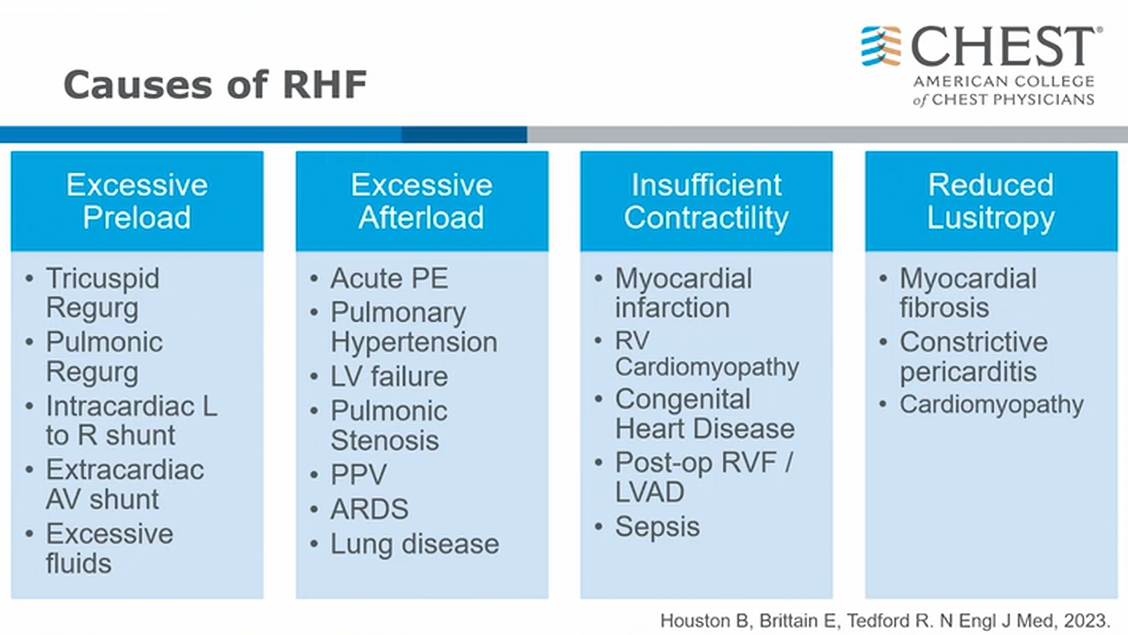
- extracardiac AV shunt: aneurysmal dialysis shunt with lots of return flow
- PPV: positive pressure ventilation
- mechanical support can cause RV failure
Management Overview
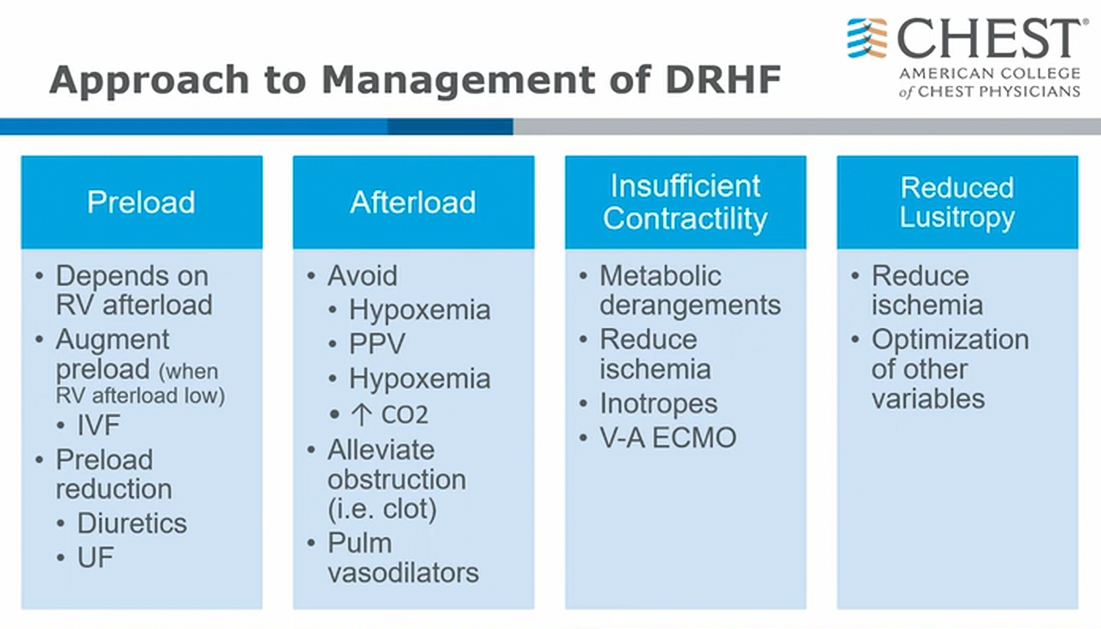
- in RV infarct, where afterload to RV should be normal, RV could be preload dependent and could be appropriate to give volume
- most cases are elevated afterload and removal of volume is needed to optimize preload
- elevated CO2 can cause further pulmonary vasoconstriction
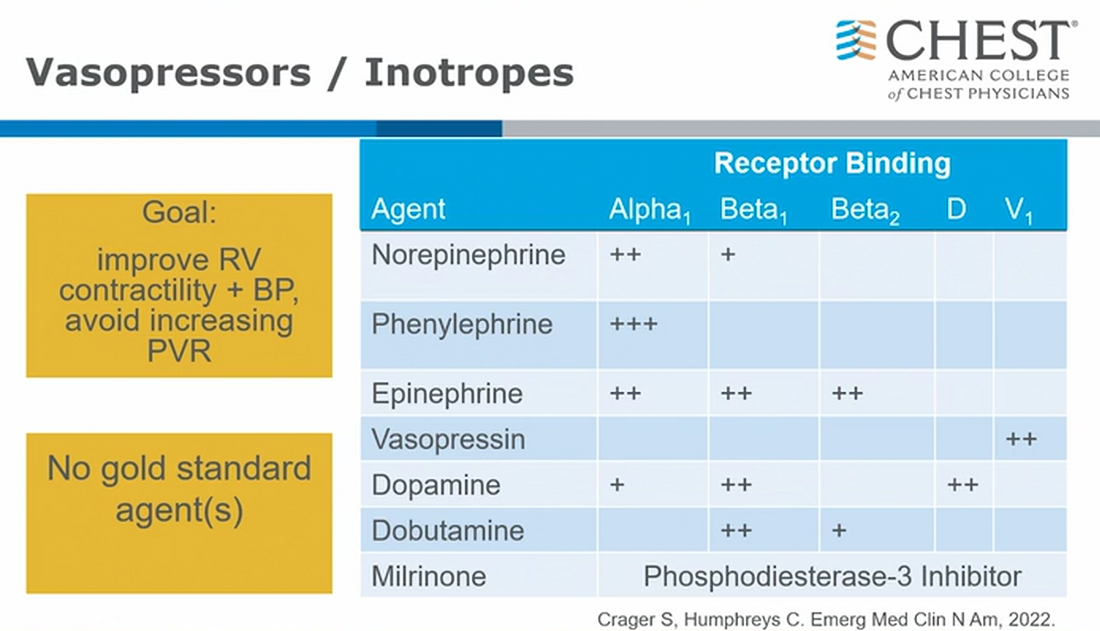
- epi used after cardiac surgery for RV
- no real literature support
- vasopressin most ideal, elevated SVR without increase PVR
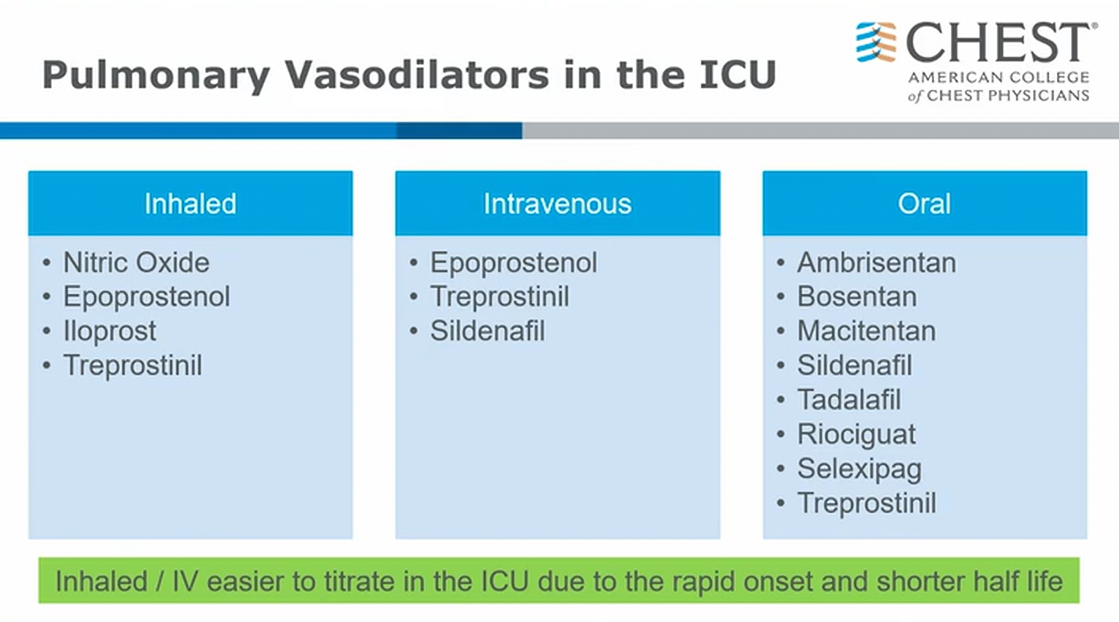
- inhaled NO and Epoprostenol are typically used for high RV afterload but also sometimes used for patients with refractory severe hypoxemia
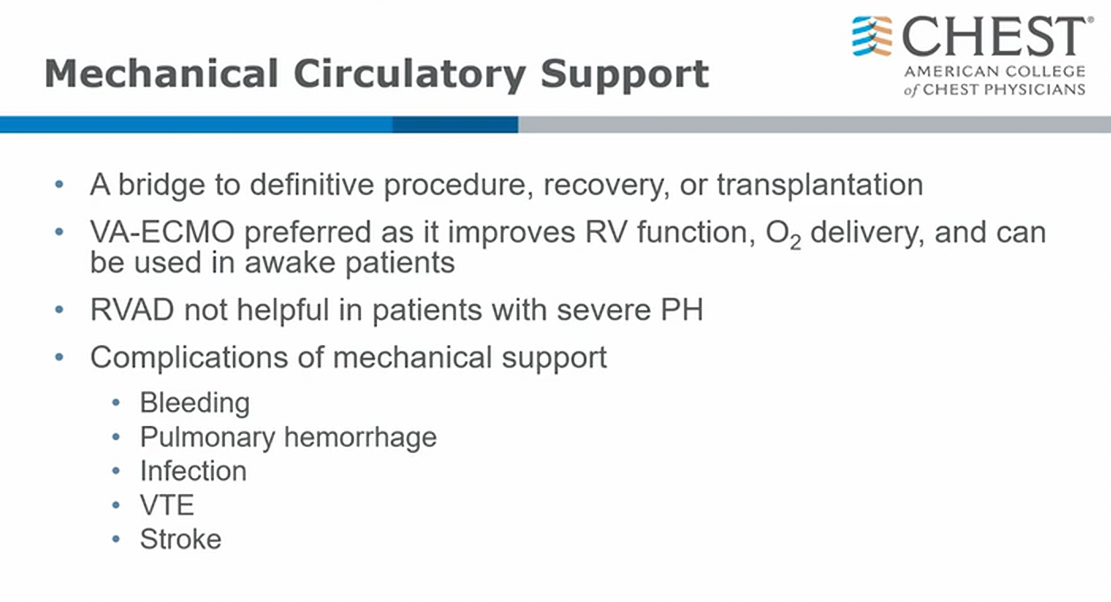
- RVAD cannot handle high afterload in pulmonary circulation
- RVAD can be used in RV failure related to LV failure or post cardiac surgery RV failure => normal or close to normal PVR
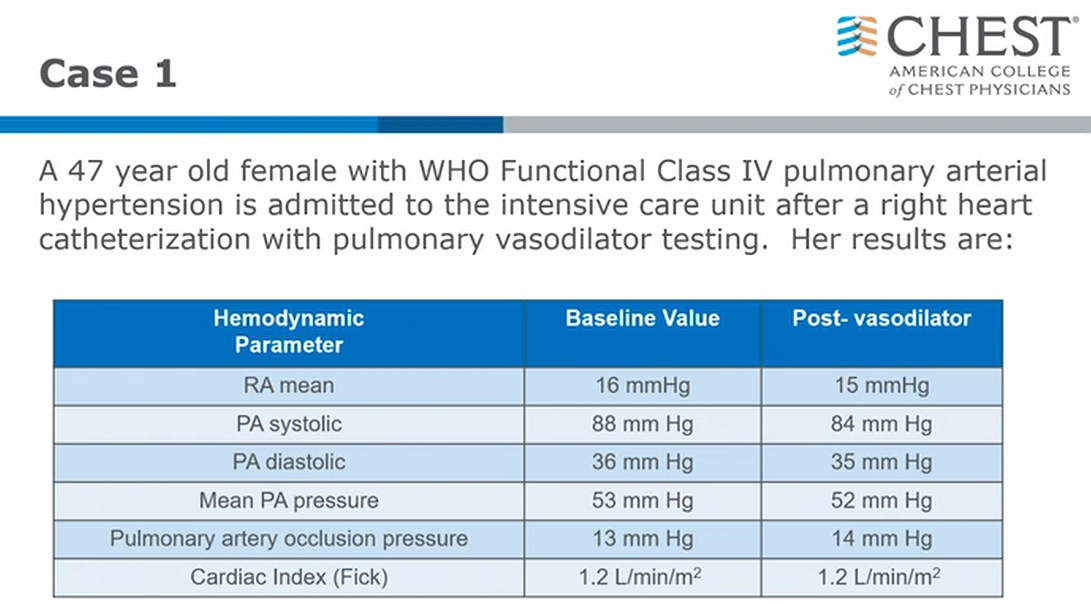
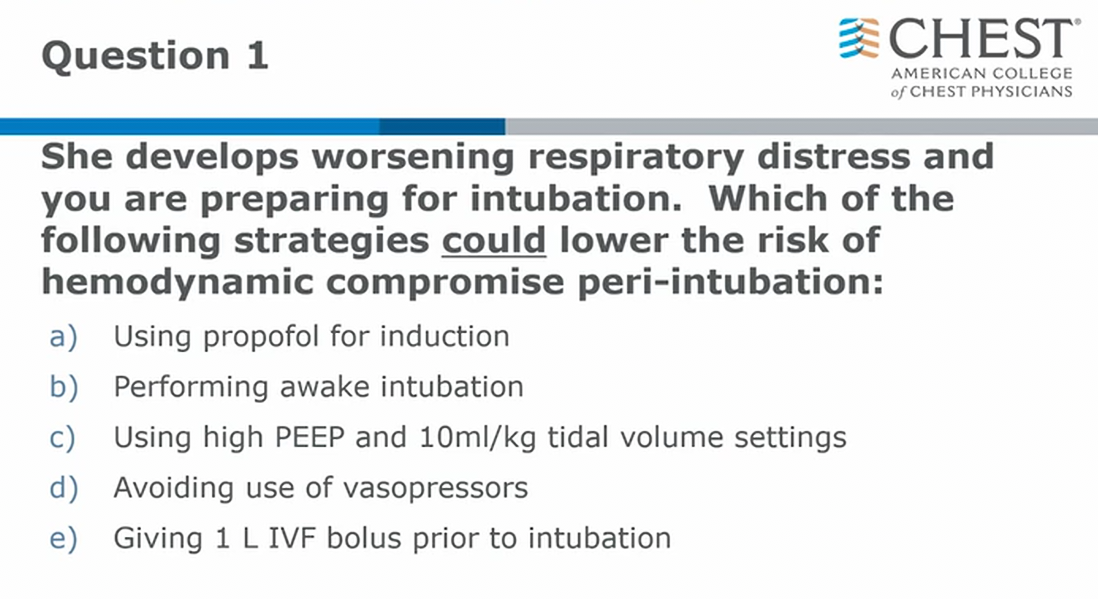
Intubations
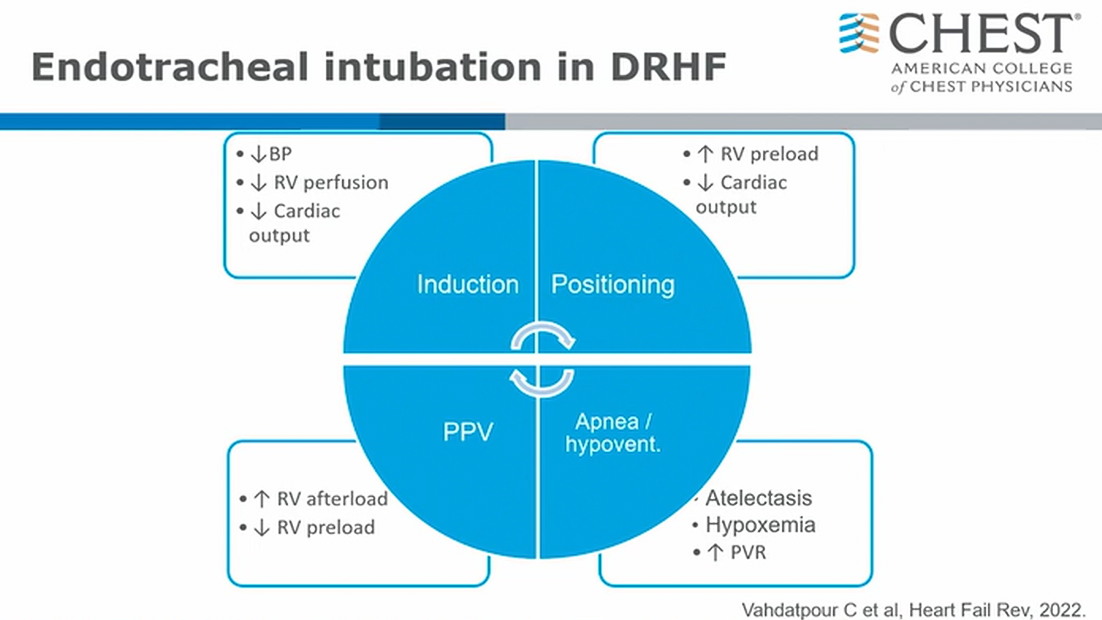
- RV decompensates with intubation
- Lower BP can lead to further RV ischemia
 1
1
Links to this note