esophageal rupture
- related: elevated amylase in pleural effusion suggests esophageal rupture or pancreatitis
- tags: #literature #pulmonology #icu
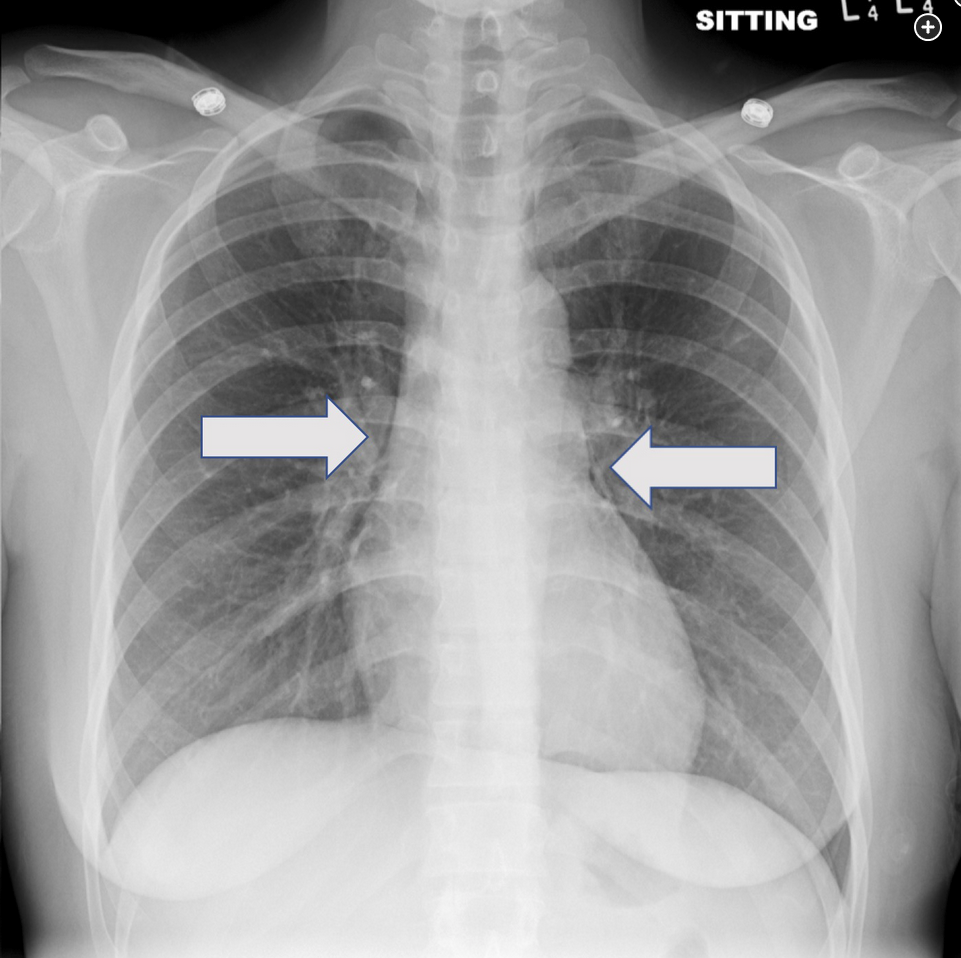
This patient’s chest radiographs reveal a pneumomediastinum, which in the clinical context of protracted vomiting raises reasonable concern for esophageal rupture (Boerhaave’s syndrome). Assessment for possible esophageal leak by fluoroscopic study would be the next appropriate step. When this study was performed (Figure 6), an esophageal leak was identified, and the patient was taken for emergent surgical repair. CT scanning can also be helpful to determine the extent of injury.
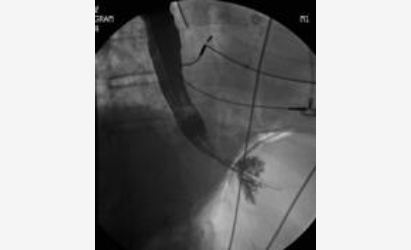
- Fluoroscopic esophageal study revealing dye extravasation.
Spontaneous esophageal rupture can occur during forceful retching and often presents acutely with vomiting, chest pain, and subcutaneous emphysema (Mackler’s triad) or some other manifestation of barotrauma in the chest (as in this case). Severe vomiting in an alcoholic is a common setting for injury. In the great majority of cases, the esophageal tear is linear, located in the distal esophagus just above the gastroesophageal junction, and in a posterolateral position. Given this location, left pneumothorax may be seen on the chest radiograph, and as the contaminated mediastinal and pleural spaces progress with infection, left pleural effusion is common. If thoracentesis is performed, the pleural fluid is exudative, with a low pH and extremely high amylase level, the latter related to saliva spillage. Once mediastinal and pleural infection become entrenched, which happens quickly, sepsis and high mortality characterize this process. Accordingly, early diagnosis and repair are imperative. In most cases, definitive repair by thoracotomy is pursued, but in some cases stenting via endoscopy is an option.12345
Links to this note
-
elevated amylase in pleural effusion suggests esophageal rupture or pancreatitis
- elevated amylase in pleural effusion can be from esophageal rupture or pancreatitis
-
- related: GI gastroenterology, esophageal rupture
Footnotes
-
de Schipper JP, Pull ter Gunne AF, Oostvogel HJ, et al. Spontaneous rupture of the oesophagus: Boerhaave’s syndrome in 2008. Literature review and treatment algorithm. Dig Surg. 2009;26(1):1-6. PubMed ↩
-
Persson S, Rouvelas I, Irino T, et al. Outcomes following the main treatment options in patients with a leaking esophagus: a systematic literature review. Dis Esophagus. 2017;30(12):1-10. PubMed ↩
-
Shaker H, Elsayed H, Whittle I, et al. The influence of the ‘golden 24-h rule’ on the prognosis of oesophageal perforation in the modern era. Eur J Cardiothorac Surg. 2010;38(2):216-222. PubMed ↩
-
Watkins JR, Farivar AS. Endoluminal therapies for esophageal perforations and leaks. Thorac Surg Clin. 2018;28(4):541-554. PubMed ↩