febrile neutropenia
- related: Hematology, Oncology
- tags: #literature #hemeonc
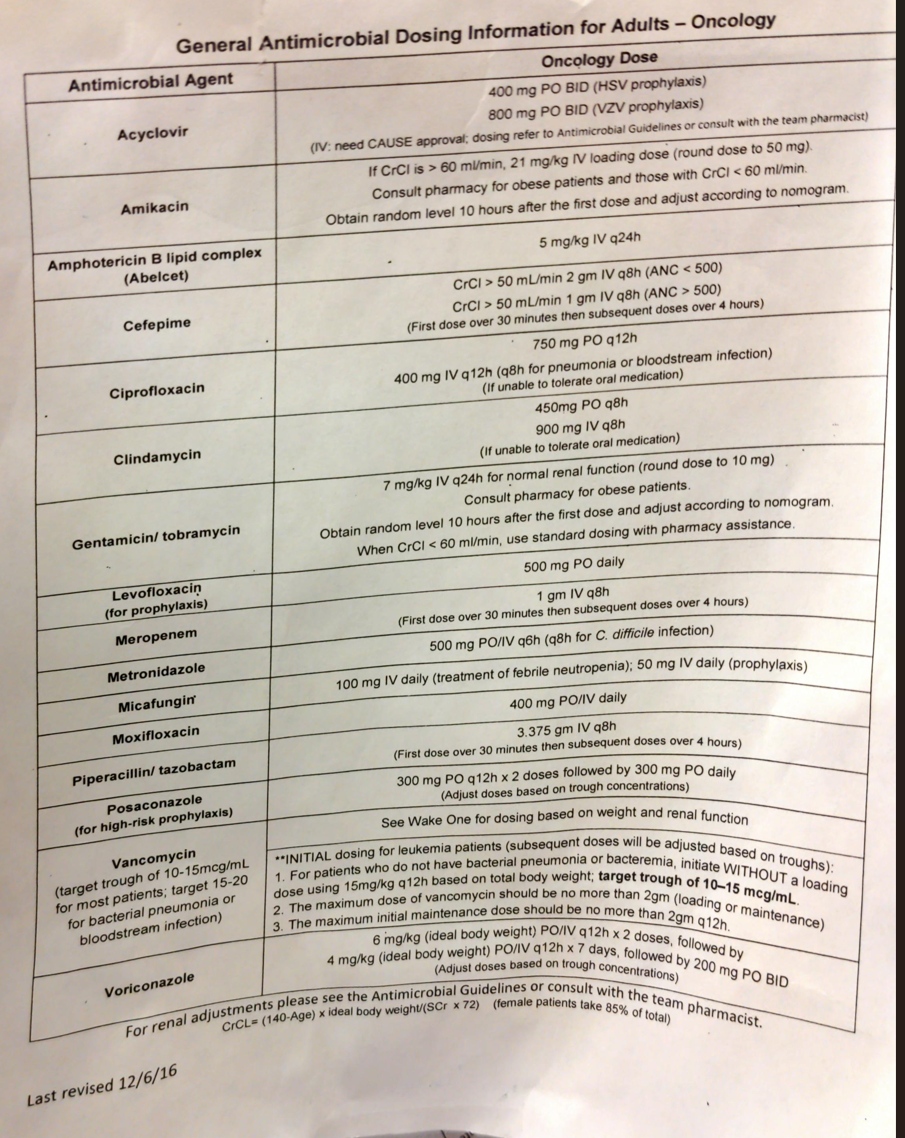
Neutropenic prophylaxis
- antiviral: acyclovir if HSV+
- antifungal
- fluconazole if on cytarabine/venetoclax
- posaconazole if on 7+3, cytarabine/daunorubicin/midaustaurin
- antibacterial
- moxifloxacin inpatient
- levofloxacin ambulatory
- maintain gram negative coverage until ANC resolves
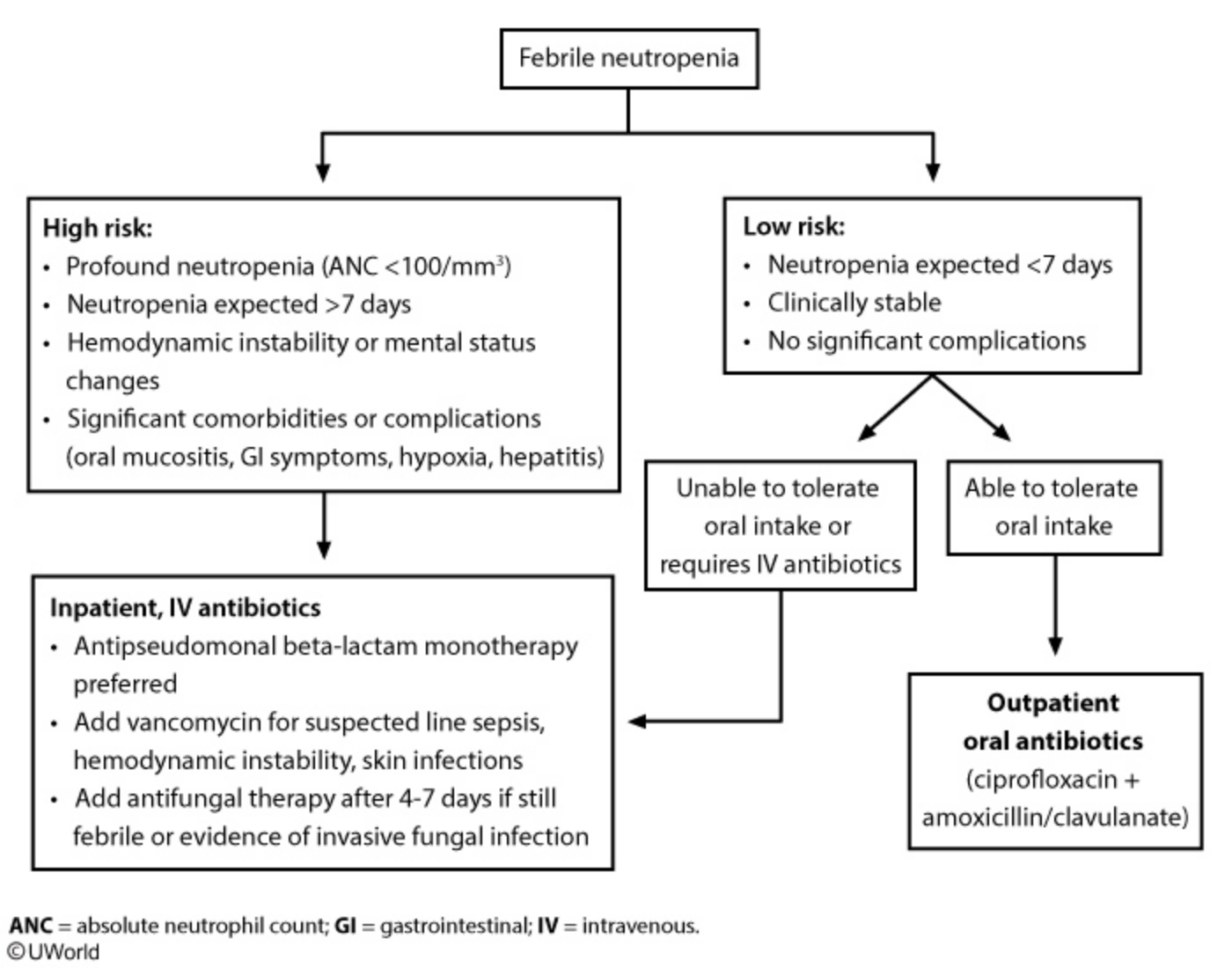
Febrile neutropenia is generally defined as a temperature >38.3 C (>101 F) and an absolute neutrophil count <500/mm3. Most cases are due to gram-positive pathogens such as Staphylococcus epidermidis (most common), Staphylococcus aureus, and streptococci, but gram-negative bacteria (eg, Pseudomonas) are isolated in approximately 25% of cases and are often associated with more severe illness.
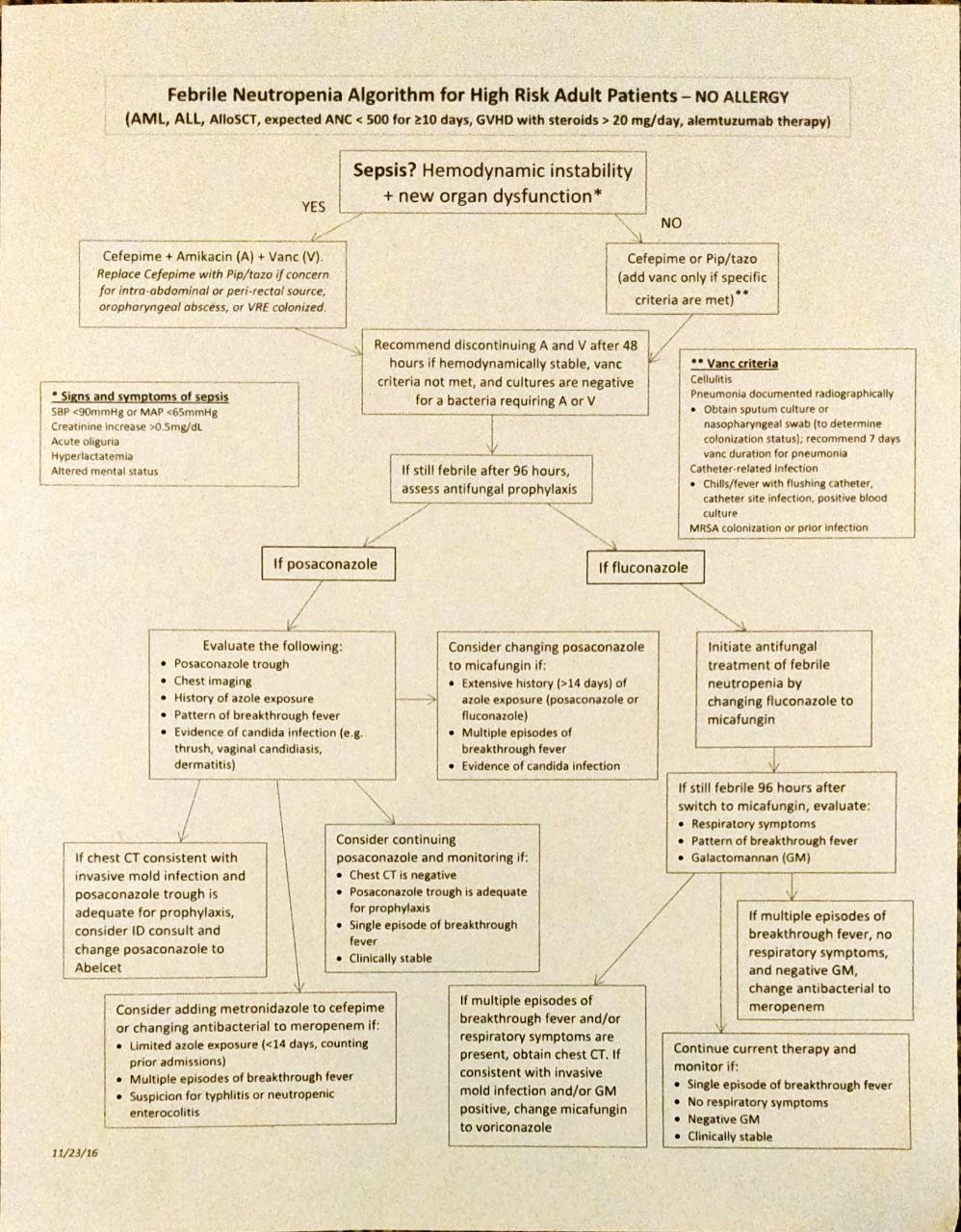
Monotherapy with an anti-pseudomonal beta-lactam (eg, piperacillin-tazobactam, cefepime) or a carbapenem is considered first-line treatment in the inpatient setting. Studies have shown no improvement in mortality with the routine addition of a second agent (eg, vancomycin) targeting gram-positive pathogens. Indications for vancomycin include:
- Hemodynamic instability
- Severe sepsis
- Pneumonia
- Positive blood cultures for a gram-positive organism (prior to speciation results)
- Suspected catheter-related infection (eg, chills during infusion, cellulitis around entry site)
- Skin or soft-tissue infection