GLI equation how did it come about
- related: PFT and lung functions
- tags: #literature #pulmonology
The GLI was established in 2008 and became a European Respiratory Society Task Force in 2010. It has been endorsed by several societies (including the American College of Chest Physicians [CHEST]) from around the globe. A major goal was to establish an international spirometry reference equation using sophisticated statistical modelling on 73 published reference equation data sets derived from healthy nonsmokers from 26 countries (choice A is correct; choices B, C, and D are incorrect).
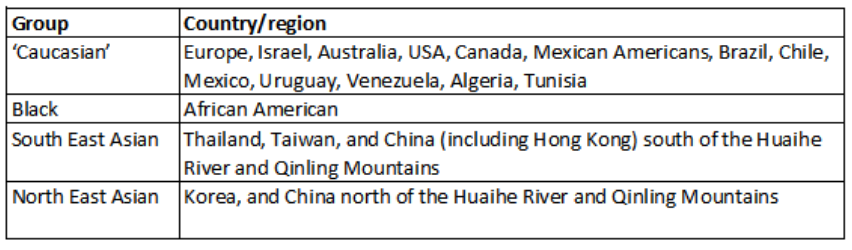
Using data from >73,000 healthy nonsmokers, the GLI equations were generated using a methodology known as lambda, mu, sigma (LMS) that better accounts for the factors that influence growth and decline in lung function, and that has been used previously to generate growth charts. Spirometry prediction equations and lower limits of normal (LLN) for FVC, FEV1, and the FEV1/FVC ratio were established for four racial/ethnic groups (Caucasian, black [African American]), North East Asians, and South East Asians, aged 3-95 years). These groups are defined in Figure 1 :
Although the GLI equations are quite similar for Caucasian and African American groups to the equations for those groups in the large US National Health and Nutrition Examination Survey III database, many laboratories are adopting the GLI formulae to standardize spirometric results around the globe. The next GLI project will use similar methodologies to produce international reference equations for Dlco.
Age, sex, and standing height were all important components of the equations. The analysis confirmed that there are proportional differences in pulmonary function among these racial/ethnic groups, reflecting effects on lung size due to differences in body build. Importantly, the FEV1/FVC ratio is generally independent of racial/ethnic group, and allows a uniform definition of airflow limitation based on the LLN for FEV1/FVC.1