hepatic vein thrombosis or Budd Chiari
- related: GI gastroenterology
- tags: #literature #GI
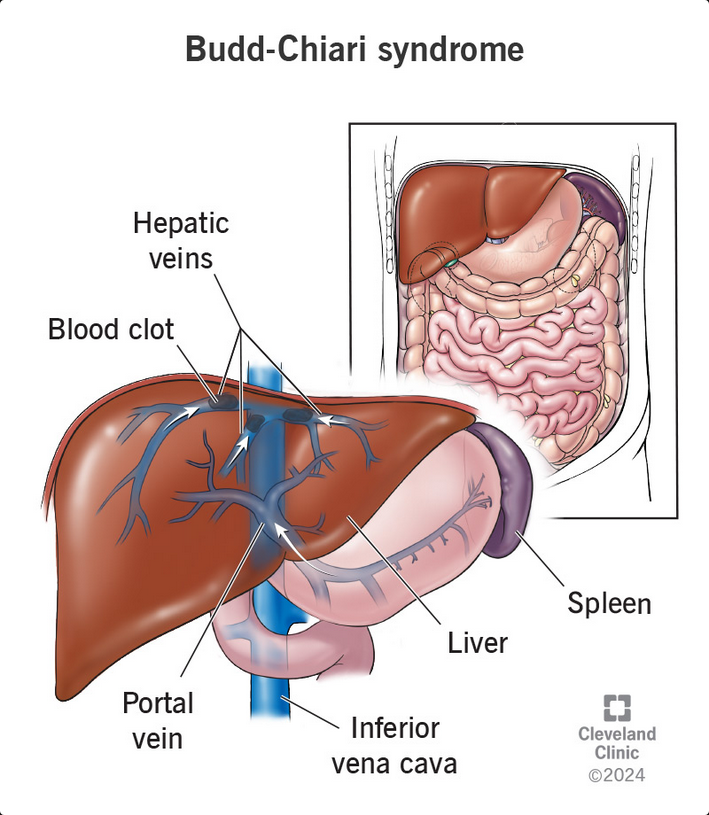
This patient has developed acute Budd-Chiari syndrome (BCS), hepatic venous outflow obstruction not due to passive causes such as cardiac disease. Primary BCS is defined as venous obstruction due to occlusion of any of the three major hepatic veins or the inferior vena cava, usually due to thrombosis, and secondary BCS is due to extrinsic mechanical or invasive causes such as compression or invasion from an extrinsic lesion. In this patient, the BCS is likely due to hepatic vein thrombosis from hypercoagulability related to an oral contraceptive agent. The thrombus or obstruction can be easily diagnosed with Doppler ultrasonography with duplex flow analysis of the hepatic vasculature, which is the best test to confirm this diagnosis.
BCS can be acute with acute hepatic failure in about 5% of patients, acute with rapidly worsening liver disease but not yet hepatic failure in about 20% of patients, subacute (developing over 2-3 months), and chronic manifesting with cirrhosis. The latter forms are likely slower in onset because of collateral venous formation. The typical patient presentation of acute BCS includes RUQ pain, abdominal distension, jaundice, ascites, hepatomegaly, and sometimes GI bleeding if varices have formed. Other findings may include edema, fever, and rarely hepatic encephalopathy. The pathophysiological characteristics are hepatic vein thrombosis leading to acute liver congestion and painful hepatomegaly due to trapped blood in the liver. Liver congestion then leads to acute hepatic necrosis and liver enzyme elevation and can progress to acute hepatic failure, acutely, or cirrhosis, chronically.
Hormonal causes of hypercoagulability, such as oral contraceptive use, as in this case, and current or recent (within 2 months) pregnancy, account for 20% of cases of BCS. The oral contraceptive use can be as short as 2 weeks. Other causes of BCS include hypercoagulability from diseases such as myeloproliferative disorders (eg, polycythemia vera and essential thrombocytosis) and account for up to 25% to 50% of cases in some series; systemic diseases such as systemic lupus erythematosus, antiphospholipid syndrome, inflammatory bowel disease and Behcet; and inherited hypercoagulable disorders such as Factor V Leiden disease, thalassemia, and protein C or S deficiency. BCS can also result from space-occupying lesions such as malignancies (accounting for 10% of cases), most commonly hepatocellular carcinoma, benign space-occupying liver lesions, and infections such as liver abscesses. On careful evaluation, a clear cause can be found in the majority (>80%) of cases of BCS.
Although abdominal ultrasonography with Doppler is the gold standard for the initial evaluation of BCS, CT scanning with contrast material and MRI can also be helpful in making this diagnosis. Noncontrast-enhanced abdominal CT scanning, perhaps considered in this case given the renal insufficiency presumably due to dehydration, would not reveal the diagnosis because it would not provide the necessary images of the hepatic vasculature.
Treatment goals for BCS are aimed at preventing clot propagation, opening the closed vessel if possible, relieving the hepatic congestion, and managing any liver failure-related complications. First-line therapy in BCS is usually anticoagulation with low-molecular-weight heparin or unfractionated heparin followed by an oral anticoagulant. Any inciting drug should be discontinued. In acute cases, if there is a defined clot and after the risks and benefits are evaluated, thrombolysis can be considered. Other treatment options include angioplasty and stent placement in the hepatic vein. In refractory cases, transjugular intrahepatic portosystemic shunt or liver transplant can be considered. As part of the risk-benefit evaluation, many recommend upper endoscopy to assess for bleeding risks before thrombolysis or anticoagulation. Untreated, BCS has a poor prognosis (<10% survival at 3 years) compared with 5-year survival rates of 75% when appropriately diagnosed and treated.
Acetaminophen, followed by amoxicillin/clavulanate, are among the most common causes of drug-induced liver disease, but 3 days is usually too soon for this to occur, the enzymes are too elevated and hepatomegaly is not typical with this form of drug-induced liver disease, and thus observation off amoxicillin/clavulanate alone would not be appropriate. Liver biopsy would likely show stages of hepatic necrosis without confirming a cause of the liver failure.1234567
A 27-year-old woman presents to the ED with severe right upper quadrant (RUQ) pain, nausea, and vomiting for 3 days. For the few days prior, she noted malaise, decreased appetite, and some upper respiratory-like symptoms and had started amoxicillin/clavulanate. Her family reports that she has seemed slightly confused for the last few hours. She does not drink alcohol and reports no recent over-the-counter acetaminophen ingestion. Her medications include an oral contraceptive agent. On examination, her temperature is 38.2°C, BP is 100/60 mm Hg, and pulse is 112/min. She is mildly icteric, and her abdominal examination is notable for distension and marked RUQ tenderness. Neurologic exam is nonfocal. Abdominal ultrasonography reveals small nonobstructing gallstones, marked hepatomegaly, an echogenic liver, and a small amount of ascites. Her laboratory test results are shown in Figure 1. Acetaminophen level and pregnancy test are negative. A hepatitis panel is pending. Ceftriaxone and normal saline are administered, and the amoxicillin/clavulanate is discontinued.
What is the best next step in her treatment?
Links to this note
Footnotes
-
Darwish Murad S, Plessier A, Hernandez-Guerra M, et al; EN-Vie (European Network for Vascular Disorders of the Liver). Etiology, management, and outcome of the Budd-Chiari syndrome. Ann Intern Med. 2009;151(3):167-175. PubMed ↩
-
Goel RM, Johnston EL, Patel KV, et al. Budd-Chiari syndrome: investigation, treatment and outcomes. Postgrad Med J. 2015;91(1082):692-697. PubMed ↩
-
Northup PG, Garcia-Pagan JC, Garcia-Tsao G, et al. Vascular liver disorders, portal vein thrombosis, and procedural bleeding in patients with liver disease: 2020 practice guidance by the American Association for the Study of Liver Diseases. Hepatology. 2021;73(1):366-413. PubMed ↩
-
Parekh J, Matei VM, Canas-Coto A, et al; Acute Liver Failure Study Group. Budd-Chiari syndrome causing acute liver failure: a multicenter case series. Liver Transpl. 2017;23(2):135-142. PubMed ↩
-
Simonetto DA, Singal AK, Garcia-Tsao G, et al. ACG clinical guideline: disorders of the hepatic and mesenteric circulation. Am J Gastroenterol. 2020;115(1):18-40. PubMed ↩
-
Valla DC. Budd-Chiari syndrome/hepatic venous outflow tract obstruction. Hepatol Int. 2018;12(suppl 1):168-180. PubMed ↩