hyperkalemia can cause severe bradycardia
- related: electrolyte disorders
- tags: #literature #icu
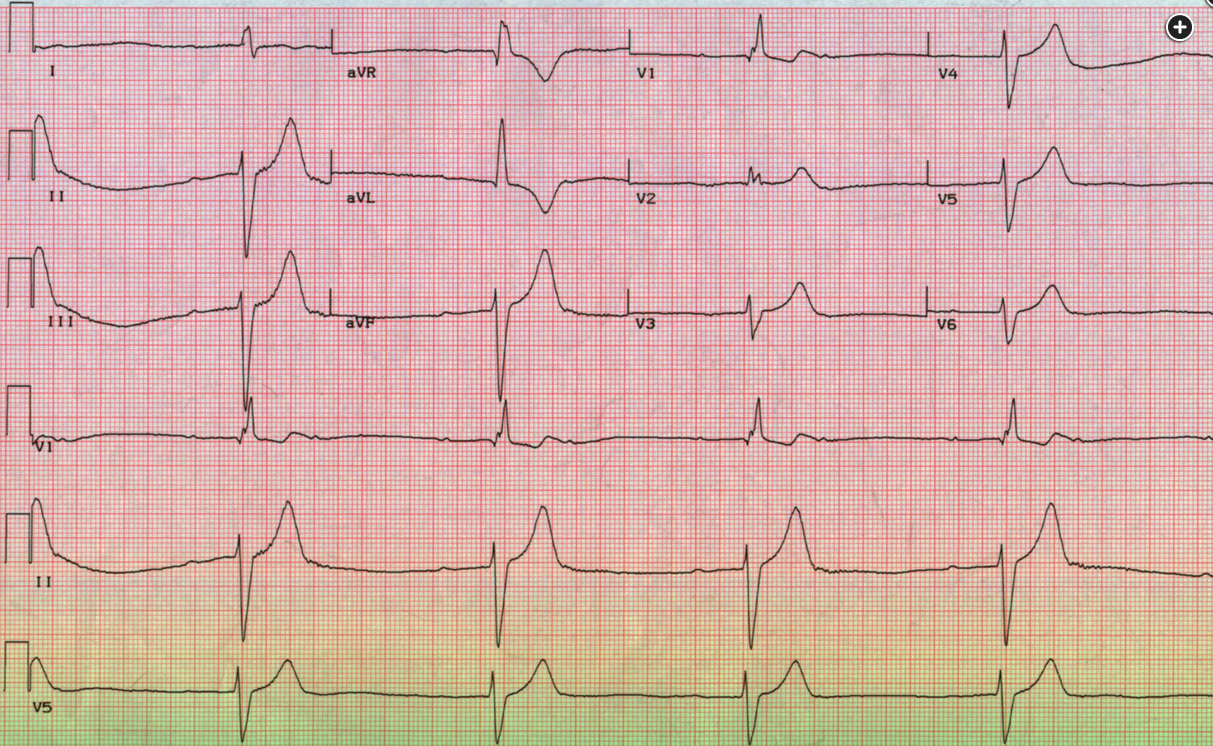
The ECG in Figure 1 shows features characteristic of hyperkalemia: peaked T waves, marked PR-interval prolongation (the P wave is actually at the end of the previous T wave), and QRS widening. The combination of these features should prompt emergency therapy for hyperkalemia even without a serum potassium level. The potassium gradient across excitable membranes is the most important determinant of resting cell membrane potential; serum hyperkalemia results in a lesser negative resting potential, with decreased conduction velocity and increased repolarization rate, which can lead to fascicular and atrioventricular nodal blocks. Untreated, hyperkalemia can progress to ventricular fibrillation or asystole.
The first step in treatment of hyperkalemic emergency, which is present based on ECG changes in this case, is stabilization of the membrane potential. This is best accomplished with IV administration of calcium, which makes the membrane potential more negative, counteracting the effects of hyperkalemia. Either calcium gluconate or calcium chloride can be given; calcium chloride is more potent but more prone to cause venous phlebitis when given peripherally (choice D is correct).
The next step is usually redistribution of potassium into the intracellular space, which can be done with insulin (given along with glucose to prevent hypoglycemia) or β2-agonists. Membrane stabilization is more important and is indicated prior to redistribution of potassium if ECG is abnormal. IV sodium bicarbonate has been given for this indication, but its efficacy is uncertain, especially if the patient is not acidemic to begin with. Elevation of resting membrane potential can close voltage-sensitive sodium channels, and solutions with sodium counteract this to some extent; effects of sodium bicarbonate may result as much from sodium as from bicarbonate (choice B is incorrect). There is no evidence for hypokalemia (choice C is incorrect). Empiric naloxone administration is appropriate in some settings, but there are no clinical features that suggest opiate overdose; respiratory rate is not low, and pupils are not pinpoint (choice A is incorrect).
None of these interventions affect total body potassium levels, so in most cases, they must be followed by interventions that remove potassium. Diuretics can be used but should not be the only method employed in patients with a hyperkalemic emergency. Gastrointestinal cation exchanges are effective independent of renal function. Patiromer and sodium zirconium cyclosilicate are preferable to sodium polystyrene sulfonate, because they are not only faster and more effective but also associated with fewer adverse events. Sodium polystyrene sulfonate has been associated with bowel necrosis, especially when given along with sorbitol.123