ITP immune thrombocytopenia
- related: Hematology
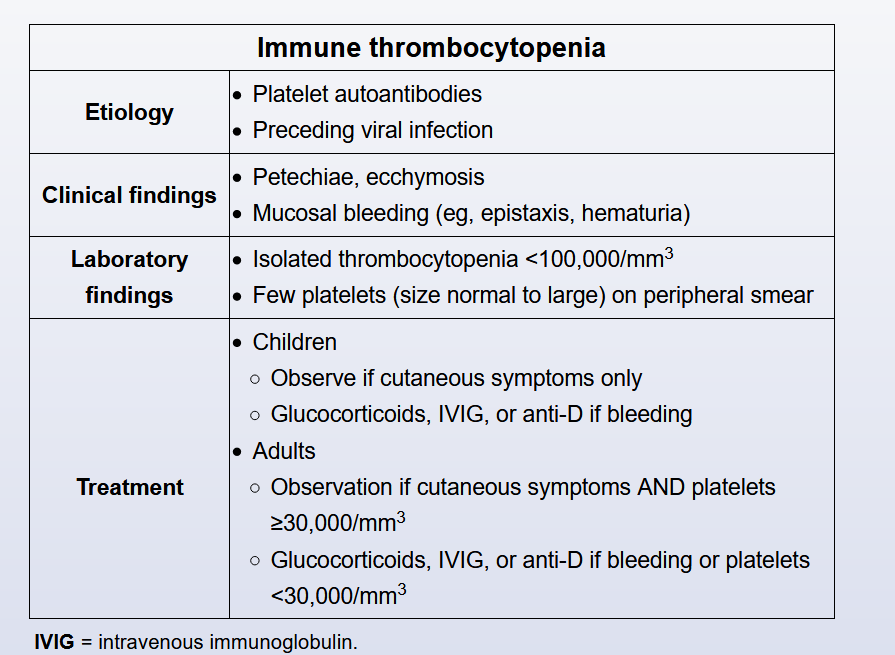
- Patients with asymptomatic mild thrombocytopenia (platelets >30,000/µL without bleeding) can generally be observed without treatment.
- Corticosteroids are a first-line treatment option for patients with symptoms and/or a platelet count of <30,000/µL; the majority of adults respond within 1-2 weeks.
- Intravenous immunoglobulin can be considered in patients who have failed or have contraindications to steroid therapy or require a more rapid increase in platelet counts.
- contrast this with TTP patients (treat TTP with plasmaphresis and steroid)
- Anti-Rh(D) is an alternate treatment option in rhesus-positive non-splenectomized patients.
- Rituximab can be considered for patients who have failed initial treatment. Splenectomy is generally reserved for refractory cases .
Links to this note
-
treat TTP with plasmaphresis and steroid
- It is rare for a patient with TTP to have the full classic pentad (fever, MAHA, thrombocytopenia, renal failure, and neurologic symptoms). The presence of MAHA and thrombocytopenia (not due to other causes) is enough to diagnose suspected TTP and initiate treatment with plasma exchange (even without fever, as in this patient). Measurement of ADAMTS13 activity is not required to make the diagnosis. Replacement of ADAMTS13 via plasma exchange stabilizes and improves most cases of idiopathic TTP. Failure to institute timely therapy can lead to devastating end-organ consequences. Initiating plasma exchange therapy while waiting for additional test results is the most appropriate next step in management. Patients refractory to plasma exchange therapy may respond to rituximab or cyclosporine. Contrast this with ITP (ITP immune thrombocytopenia)