LV overdistension in ECMO
- related: cardiac supportive devices
- tags: #literature #icu
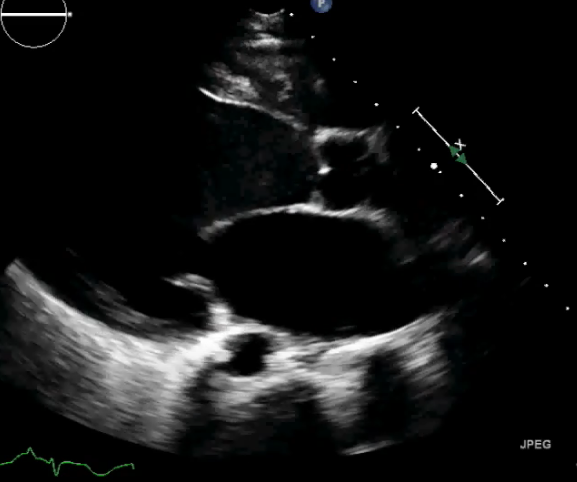
This patient is in cardiogenic shock. The echocardiogram shows severe left ventricular (LV) dysfunction and LV enlargement. A key additional finding is that the aortic valve fails to open during systole, meaning that the entire systemic blood flow derives from the ECMO circuit. The LV does not eject because it cannot develop sufficient pressure to overcome the pressure in the aortic root. This has several deleterious consequences. First, stasis in the LV outflow tract (notice the spontaneous echo contrast in the LV outflow tract) and proximal aorta risks thrombosis and systemic embolism. Second, despite not ejecting, the LV continues to fill through the pulmonary and Thebesian veins, raising LV and pulmonary vascular pressures. Ventricular overdistention produces pulmonary edema and may delay LV recovery. (If heart doesn’t pump at all, then flow from pump will make heart more distended over time).
Treatment seeks to decompress the LV and can include inotropes (such as dobutamine); intraaortic balloon counterpulsation (to reduce LV afterload); reducing the ECMO pump speed (which lowers LV afterload); placement of an LV assist device; or transvenous, transseptal cannula drainage. Reducing PEEP will tend to raise LV afterload, further impeding ejection (choice D is correct; choices A, B, and C are incorrect).
When venoarterial ECMO is used for severe LV dysfunction, roughly 50% of patients will experience LV overdistention. Therefore, it is important to monitor the arterial pulse wave (pulsatility is proportional to native stroke volume), echocardiographic signs, or pulmonary vascular pressures. Clues to LV overdistention include radiographic or ultrasonographic findings of increasing pulmonary edema, falling respiratory system compliance, increasing LV volume, and rising pulmonary artery diastolic pressure.123
Links to this note
Footnotes
-
Ricarte Bratti JP, Cavayas YA, Noly PE, Serri K, Lamarche Y. Modalities of left ventricle decompression during VA-ECMO therapy. Membranes (Basel). 2021;11(3):209. PubMed ↩
-
Rihal CS, Naidu SS, Givertz MM, et al. 2015 SCAI/ACC/HFSA/STS clinical expert consensus statement on the use of percutaneous mechanical circulatory support devices in cardiovascular care: endorsed by the American Heart Assocation, the Cardiological Society of India, and Sociedad Latino Americana de Cardiologia Intervencion; Affirmation of Value by the Canadian Association of Interventional Cardiology-Association Canadienne de Cardiologie d’intervention. J Am Coll Cardiol. 2015;65(19):e7-e26. PubMed ↩