necrotizing infections from vibrio
- related: necrotizing infections
- tags: #literature #id
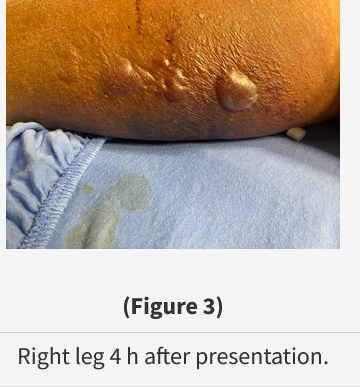
This patient is profoundly ill and presenting with signs and symptoms of necrotizing fasciitis. He has two known risk factors for necrotizing fasciitis—specifically, diabetes and cirrhosis. The diagnosis of necrotizing fasciitis is usually based on clinical suspicion and physical examination results. Limb pain initially out of proportion to skin changes and elevated creatine kinase levels are typical findings. This patient’s laboratory results are suggestive of a more severe infection than was initially apparent. Overwhelming sepsis with lactic acidosis, acute kidney injury, disseminated intravascular coagulopathy, relative leukopenia, and hypothermia portend a poor prognosis. In less apparent cases, CT imaging may show gas formation where anaerobes are present. Early surgical consultation and extensive debridement, if possible, are key to survival. Four hours after presentation, the skin of this patient’s leg showed cyanosis and extensive epidermal necrolysis (Figure 3). Despite appropriate empiric antibiotics and supportive care, he was too ill to undergo debridement and died within 12 h of presenting to the emergency department. His blood cultures (four of four bottles) returned positive for Vibrio vulnificus.
Microorganisms that may cause necrotizing fasciitis in susceptible hosts include group A streptococci, Mucorales species, Staphylococcus aureus, V vulnificus, and Clostridium species. This patient’s occupation as a crab fisherman should raise the suspicion of infection due to V vulnificus, a gram-negative bacteria that thrives in warm saltwater or brackish water. When infection occurs by eating raw or undercooked shellfish, gastroenteritis is common. Exposure via an open wound can lead to severe necrotizing fasciitis with fulminant sepsis after a short incubation period.
In unclear cases of necrotizing fasciitis, the Infectious Diseases Society of America would recommend empiric treatment with vancomycin or linezolid plus either (a) piperacillin-tazobactam or a carbapenem or (b) ceftriaxone and metronidazole. However, in the present case, V vulnificus is suspected because there has been exposure of a wound to warm brackish water or saltwater with resulting fulminant sepsis. In cases of severe V vulnificus necrotizing fasciitis, double coverage with ceftazidime and doxycycline is recommended.
Zygomycete fungal necrotizing fasciitis is an emerging infectious disease. Mucorales species are the most common isolated organisms. Zygomycetes are commonly found in the soil and can cause invasive disease if inoculated into soft tissue in a susceptible host, such as someone with diabetes, where they invade blood vessels and lead to tissue infarction. The clinical illness caused by Mucorales species, mucormycosis, most commonly involves the sinuses (rhinocerebral) or lungs. Several cases of pulmonary mucormycosis have been reported in association with COVID-19 infection. Cutaneous mucormycosis can occur in a susceptible host after direct skin inoculation. Liposomal amphotericin B and posaconazole are the antimicrobial treatments of choice for mucormycosis, but skin mucormycosis is not as fulminant as the illness presented in the script.
Clostridium tetani is an anaerobic gram-positive bacteria that produces a neurotoxin that inhibits upper motor neurons leading to disinhibition (hyperreactivity) of lower motor neurons. Although this wound is tetanus prone, the presentation of overwhelming sepsis is atypical for tetanus. The classical presentation of tetanus begins with trismus of the masseter muscles. Muscle rigidity then spreads downward over the next few days, progressing to severe generalized muscle rigidity. Autonomic instability is also a common feature. Supportive treatment may require neuromuscular blockade and mechanical ventilation. Along with wound debridement, neutralization of tetanus toxin by infiltrating human antitetanus immunoglobulin into the wound may be useful. High-dose penicillin G or metronidazole is the preferred antimicrobial. Tetanus toxoid is immunogenic and is used in vaccines to prevent tetanus, but it has no use in treating tetanus.
Mycobacterium marinum is an aerobic, weakly pathogenic photochromogenic nontuberculous bacteria found in marine and brackish waters worldwide. It typically causes nonhealing granulomatous skin infections in humans by direct inoculation. Combination clarithromycin plus trimethoprim-sulfamethoxazole is a preferred treatment. However, this stem describes a patient with fulminant sepsis, which does not fit the clinical script for M marinum infection.
S aureus only rarely causes necrotizing fasciitis, and, when it does, it is usually in the setting of cellulitis, which this patient does not have. Although empiric antistaphylococcal coverage with vancomycin is warranted, this option was not offered and would not address the most likely causative agent of this patient’s infection.1234
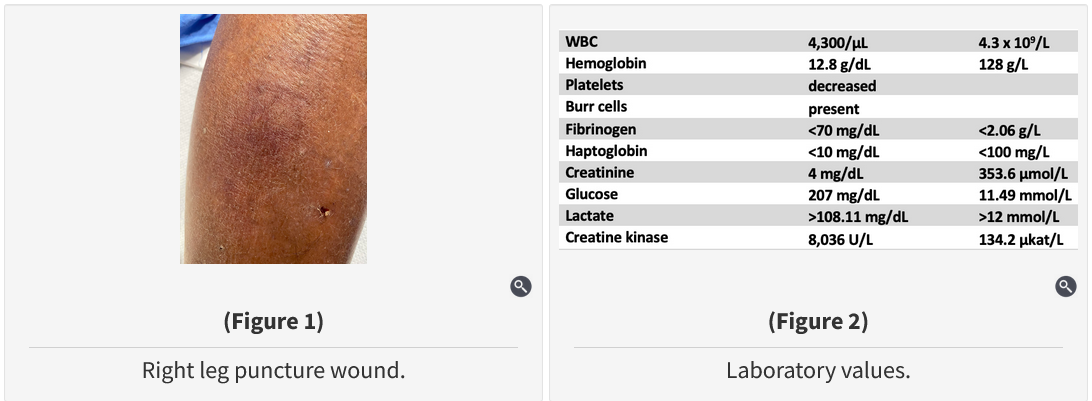
A 55-year-old Gulf Coast fisherman with a history of type 2 diabetes mellitus, cirrhosis, chronic atrial fibrillation, and nonischemic cardiomyopathy presents to the emergency department with shortness of breath and severe limb pain and stiffness 24 h after sustaining a small puncture wound to his right leg from a crab trap.
At arrival, his heart rate is 150/min and irregular, BP is 77/55 mm Hg, respiratory rate is 30/min, SpO2 is 93% breathing room air, temperature is 35.1 °C, and BMI is 35 kg/m2. On examination, he appears ill, and his breathing is labored. His lungs are clear to auscultation. There is no erythema of his legs, and his feet are warm and pink. There is a superficial 5-mm nondraining wound over the medial aspect of his right leg. His leg and thigh are exquisitely tender. A chest radiograph is normal. A photograph of his leg wound is shown in Figure 1, and initial laboratory values are shown in Figure 2.
In addition to surgical consultation and supportive measures, which of the following regimens would be indicated to treat this patient’s suspected infection?
Links to this note
Footnotes
-
Chen SC, Lee YT, Tsai SJ, et al. Antibiotic therapy for necrotizing fasciitis caused by Vibrio vulnificus: retrospective analysis of an 8 year period. J Antimicrob Chemother. 2012;67(2):488-493. PubMed ↩
-
Diab J, Bannan A, Pollitt T. Necrotising fasciitis. BMJ. 2020;369:m1428. PubMed ↩
-
Leng F, Lin S, Wu W, et al. Epidemiology, pathogenetic mechanism, clinical characteristics, and treatment of Vibrio vulnificus infection: a case report and literature review. Eur J Clin Microbiol Infect Dis. 2019;38(11):1999-2004. PubMed ↩