nocardia and actinomyces
- related: Infectious Disease ID
- tags: #literature #pulmonology
- nocardia is weakly acid fast, aerobic
- actinomyces is not acid fast, anaerobic
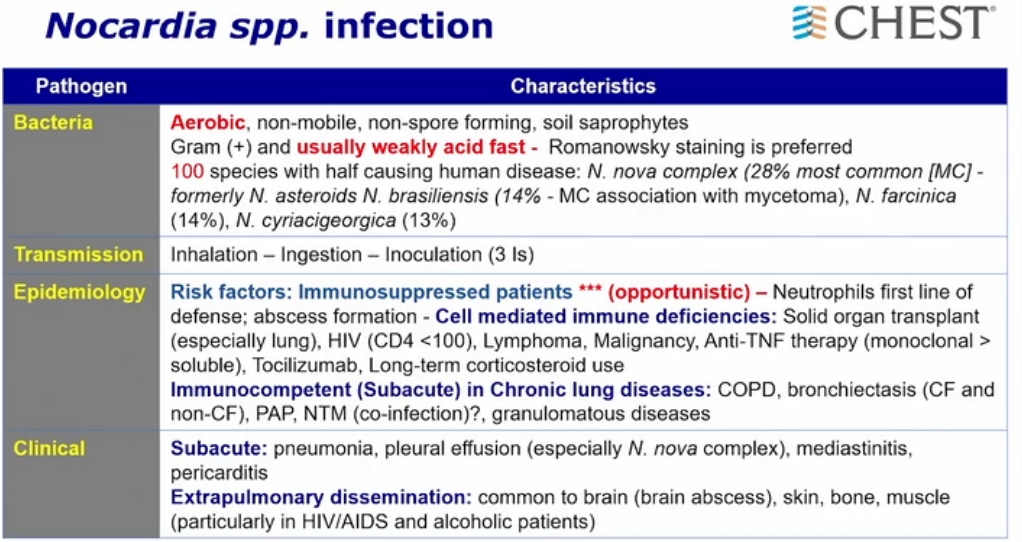
- nocardia nova complex: asteroids
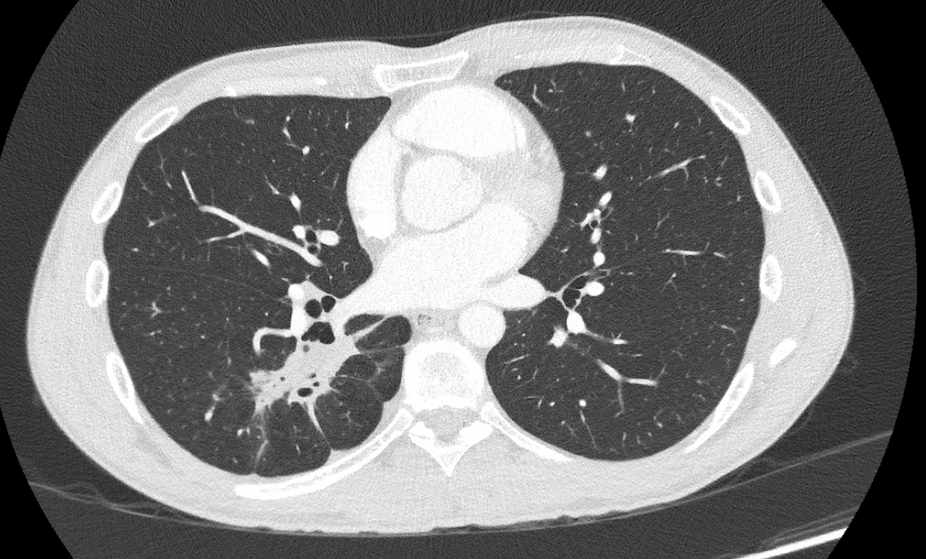
- skin lesions, lung lesions
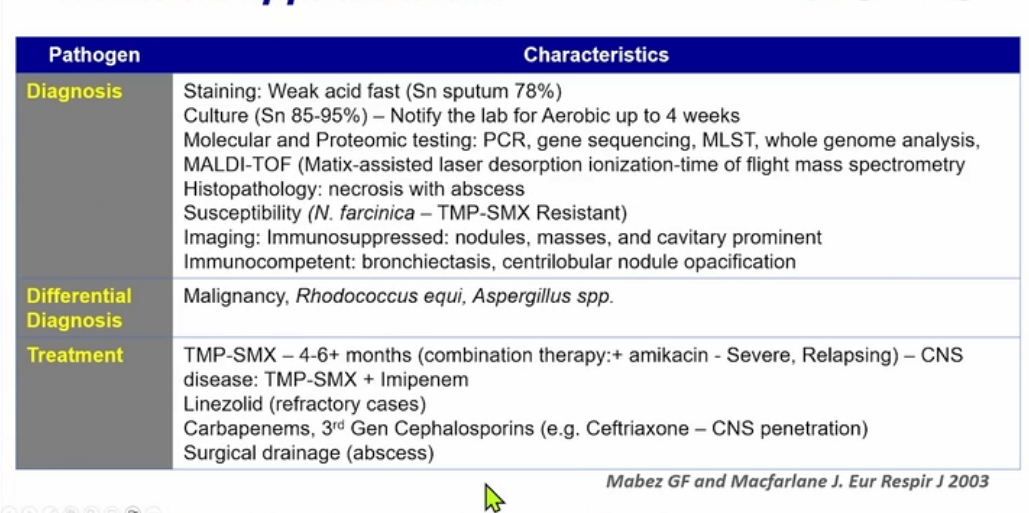
- now with PCR techniques and MALDI-TOF to identify
- may be resistant to bactrim
- For mild-to-moderate pulmonary nocardiosis in the immunocompetent host, TMP-SMX is usually the drug of choice. In the case of severe infection, and/or if there is CNS involvement, initial treatment should include 2 to 3 intravenous agents while susceptibility testing is pending, TMP-SMX plus amikacin or with the addition of imipenem for CNS disease.
- if CNS involvement use bactrim + meropenem + amikacin
- After 3 to 6 weeks of IV therapy and, depending on the response, sensitivity results, treatment can be switched to oral therapy, usually high-dose TMP-SMX. Treatment should be continued for 6 to 12 months (12 months in the immunocompromised). In patients with chronic immunosuppression, lifelong indefinite secondary prophylaxis is usually indicated. If a sulfa allergy exists, desensitization is recommended.
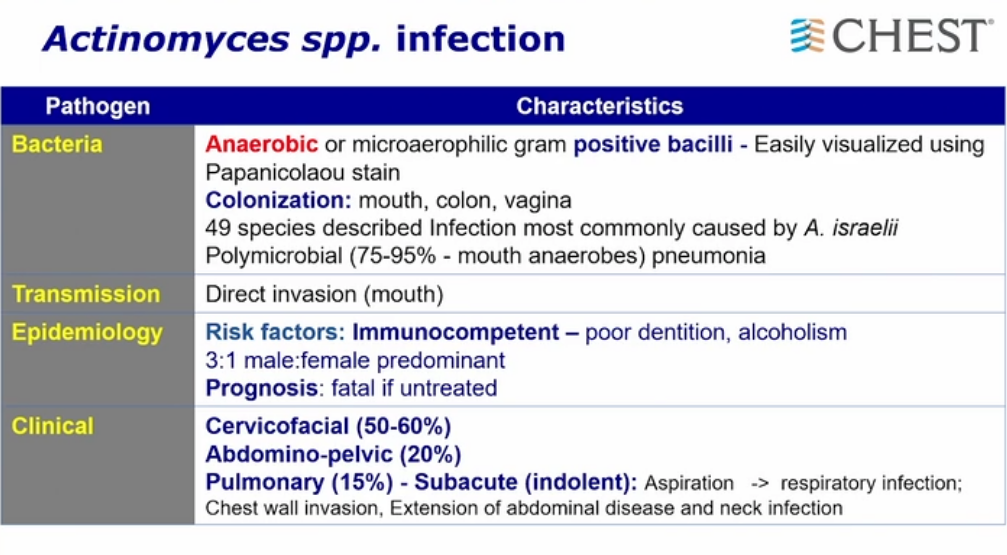
- anaerobic, beaded, branching gram positive bacteria
- immunocompentent as opposed to immunocompromised with nocardia
- can be fatal if not treated
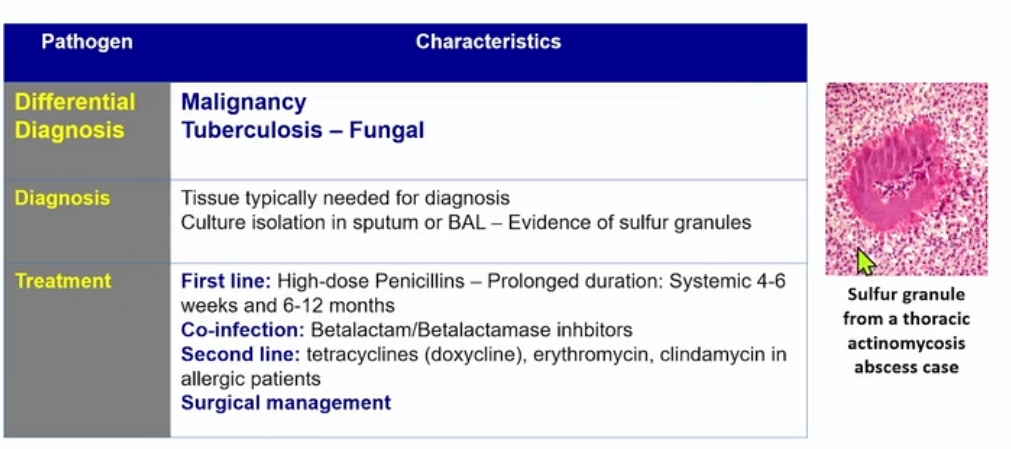
- sulfur granule pathognomonic1
- branching and filamentous gram-positive rod that does not grow aerobically on blood or Sabouraud agar and is not acid fast with routine or modified staining
- identical gram stain to Nocardia but will not grow aerobically and not acid fast staining2
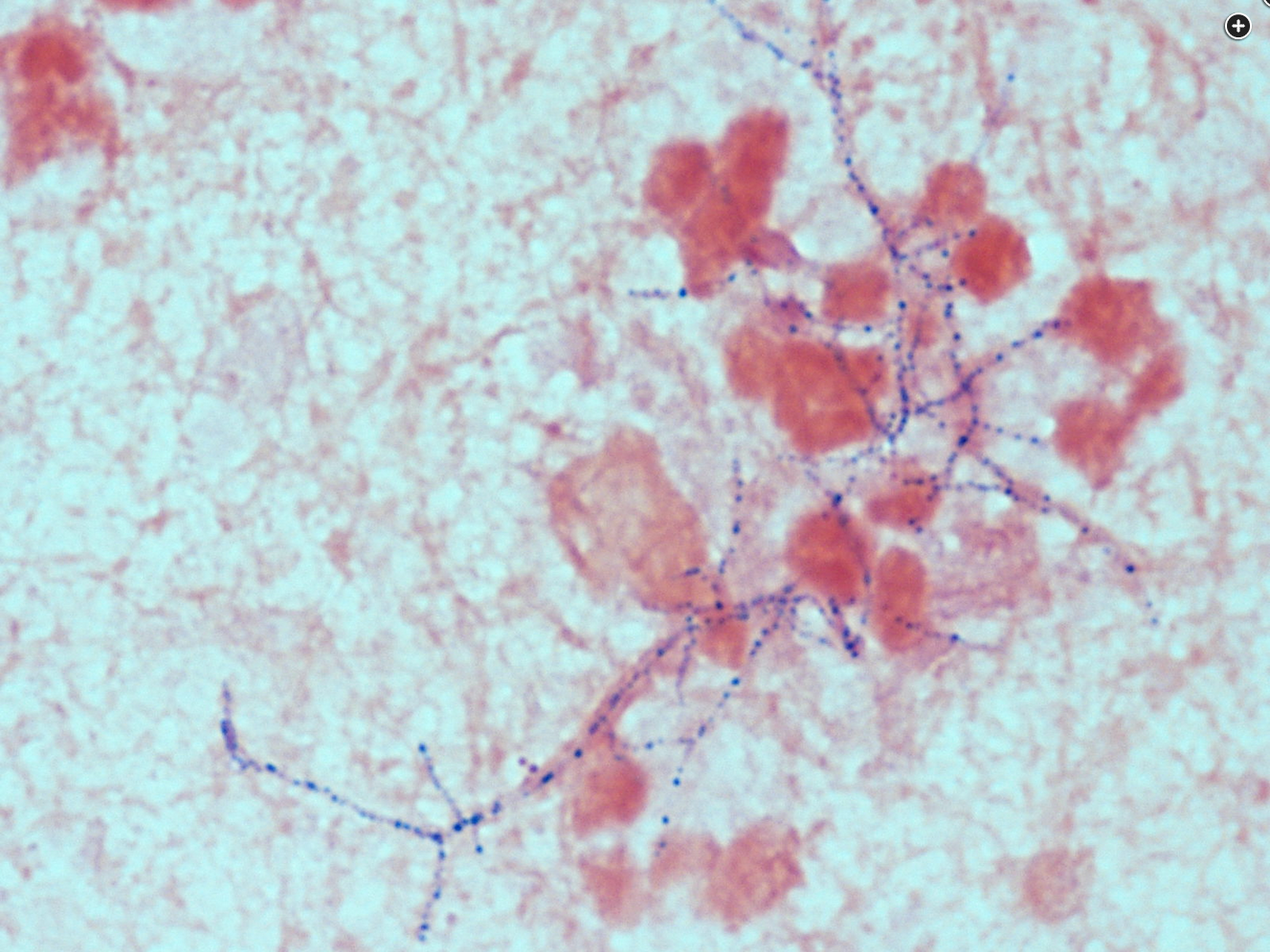
- nocardia gram stain

- actinomyces