Ogilvie syndrome aka colonic pseudoobstruction
- related: GI gastroenterology
- tags: #GI #literature #icu
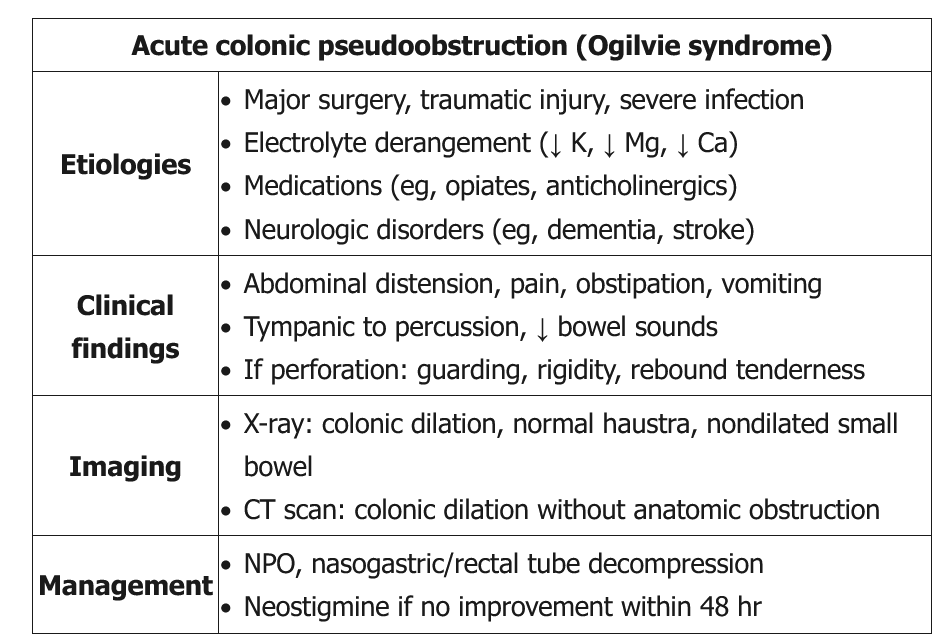
Ogilvie syndrome is most common in hospitalized or institutionalized men age >60. Although its etiology is unclear, it is suspected to be related to autonomic nervous system dysfunction in the setting of prior insults (eg, trauma, surgery, infection, neurologic disorders), particularly in combination with metabolic abnormalities (eg, hypokalemia, hypomagnesemia) or inciting medication (eg, narcotics). Patients typically have abdominal distension, pain, nausea/vomiting, constipation, or diarrhea. Examination commonly reveals a distended abdomen with increased tympany, mild tenderness, and active bowel sounds; peritoneal signs are suggestive of perforation.
CT scan is diagnostic and can differentiate Ogilvie syndrome from mechanical obstruction (presence of transition point) and toxic megacolon (thickened colonic wall with thumbprinting). Treatment is initially supportive. Serial abdominal examinations and x-rays should be performed to evaluate for perforation. In addition, management includes nasogastric tube decompression, treatment of possible underlying causes (eg, electrolyte imbalances, narcotic cessation), and early ambulation.
Neostigmine is indicated in patients who fail 24-48 hours of conservative therapy and in those with a cecal diameter >12 cm. It can lead to bradycardia, bronchospasm, and hypotension and is contraindicated in those with certain cardiovascular risk factors (recent myocardial infarction, bradycardia, beta blocker therapy), active bronchospasm, or peptic ulcer disease (Choice B). Patients who fail neostigmine or have contraindications may require colonoscopic or surgical decompression, including a percutaneous tube cecostomy.
This patient’s presentation is highly consistent with acute colonic pseudo-obstruction, or Ogilvie’s syndrome, and the degree of colonic distension warrants urgent treatment with neostigmine. This acetylcholinesterase inhibitor increases parasympathetic tone and, hence, bowel motility; however, some patients will experience bronchospasm and/or bradycardia, and agents to address these acute effects should be readily available, including albuterol and atropine (choice A is correct).
Acute colonic pseudo-obstruction is defined as acute dilation of the colon in the absence of a mechanical obstruction. This dilation usually involves the cecum and ascending colon. Common risk factors include advanced age, recent surgery, opiate use, and bed rest, all present in this patient. Cesarean section and hip surgery have the highest reported incidences of this postoperative complication, occurring most often in the first week after surgery.
The primary danger of this process is bowel dilatation leading to ischemia and perforation. Perforation becomes a significant risk when cecal diameter exceeds 10 to 12 cm. The American Society for Gastrointestinal Endoscopy and the American Society of Colon and Rectal Surgeons recommend that when Ogilivie’s syndrome is suspected, initial definitive imaging should be performed to exclude mechanical obstruction. CT scanning serves this purpose well and stratifies patients at greatest risk for bowel ischemia and/or perforation. When colonic distension is less than 12 cm and abdominal pain mild to moderate, supportive therapy alone (treatment of underlying disorders and electrolyte abnormalities, discontinuation of drugs that impair bowel motility, nasogastric decompression, enemas) should be used. When cecal dilatation is 12 cm or more or conservative therapy has failed, neostigmine is recommended unless contraindications exist (recent myocardial infarction, severe active asthma, preexisting bradycardia or heart block, preexisting use of β-blockers). Throughout conservative management or during administration of neostigmine, frequent abdominal examinations should be performed and laboratory testing conducted to monitor for possible early bowel perforation. When neostigmine cannot be used, colonoscopic decompression is a reasonable alternative. Allergic, anaphylactic, or anaphylactoid reactions to neostigmine are exceedingly rare, and treatment with corticosteroids and antihistamines is not likely to be needed (choice B is incorrect).
When circulatory effects of neostigmine are seen, they are dominated by sinus bradycardia and/or heart block and possibly hypotension related to bradycardia. Amiodarone, calcium channel blockers, and β-blockers would all be contraindicated in this setting (choices C and D are incorrect).123456
Links to this note
Footnotes
-
Alavi K, Poylin V, Davids JS, et al. The American Society of Colon and Rectal Surgeons clinical practice guidelines for the management of colonic volvulus and acute colonic pseudo-obstruction. Dis Colon Rectum. 2021;64(9):1046-1057. PubMed ↩
-
Liu JJ, Venkatesh V, Gao J, et al. Efficacy and safety of neostigmine and decompressive colonoscopy for acute colonic pseudo-obstruction: a single-center analysis. Gastroenterology Res. 2021;14(3):157-164. PubMed ↩
-
Naveed M, Jamil LH, Fujii-Lau LL, et al. American Society for Gastrointestinal Endoscopy guideline on the role of endoscopy in the management of acute colonic pseudo-obstruction and colonic volvulus. Gastrointest Endosc. 2020;91(2):228-235. PubMed ↩
-
Ross SW, Oommen B, Wormer BA, et al. Acute colonic pseudo-obstruction: defining the epidemiology, treatment, and adverse outcomes of Ogilvie’s syndrome. Am Surg. 2016;82(2):102-111. PubMed ↩
-
Vogel JD, Feingold DL, Stewart DB, et al. Clinical practice guidelines for colon volvulus and acute colonic pseudo-obstruction. Dis Colon Rectum. 2016;59(7):589-600. PubMed ↩