pleural lipoma are benign nodules
- related: lung mass and cancer
- tags: #literature #mass
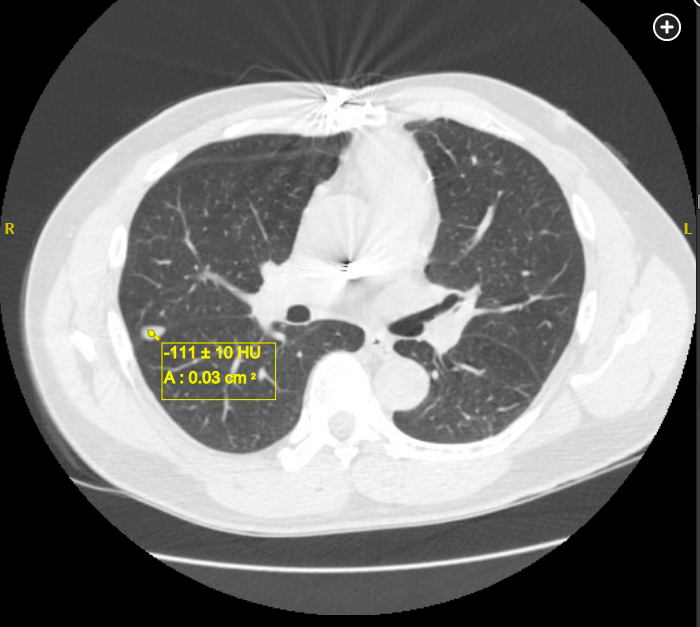
The finding on the chest CT scan is a pleural lipoma and, on the basis of its appearance, should not prompt additional short-term imaging studies, although annual screening in this patient at risk for lung cancer should continue. Pleural lipomas are slow-growing, benign tumors that are relatively common. They are derived from adipose tissue of the submesothelial parietal pleura and can extend into the subpleural, pleural, or extrapleural space. Patients commonly do not have symptoms, with the lipoma detected incidentally on CT scans performed for other purposes. Although incidentally found pleural lipomas may be small, as in this case, authors of case reports note that they are often larger, between 2 and 10 cm, with some noting even more massive sizes. If the lipoma grows large enough, symptoms including cough, dyspnea, chest pain, and dysphagia may occur owing to extrinsic compression of surrounding anatomic structures. There is no association with subcutaneous lipomas.
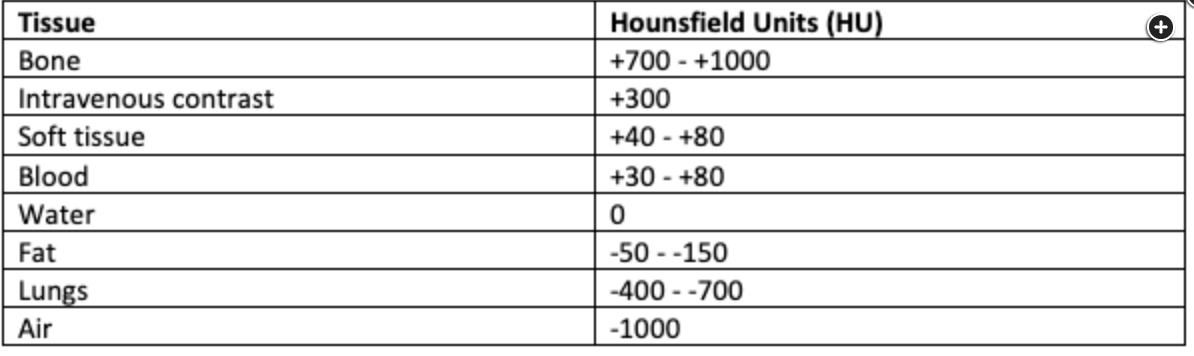
Diagnosis can usually be established by means of CT scan. Typically, pleural lipomas are described as a rounded, completely homogeneous density of fat attenuation (between −50 and −150 Hounsfield units) (Figures 2 and 3), without any calcification, and do not enhance with contrast material. The presence of calcium along with fat may suggest the diagnosis of a hamartoma, another intrathoracic benign tumor that can be diagnosed by means of a routine CT scan. Attenuation coefficients higher than −50 Hounsfield units and a heterogeneous constitution with intralesional nodular tissue, especially with contrast enhancement, or invasion of neighboring anatomical structures, raises the suspicion for a liposarcoma. In such cases, fluorodeoxyglucose PET scanning and core needle aspiration should be considered.
Clinical observation and periodic surveillance are usually suggested for those with typical CT findings, without symptoms, and without involvement of local anatomical structures, because pleural lipomas are typically slow growing without malignant transformation. Surgical resection is the treatment of choice for lesions that cause symptoms, with some advocating for early surgical intervention when lesions are large, because the surgical procedure is easier if performed before tissue infiltration. Recurrent lipoma arising from a resected margin has been reported. The patient described here remains without symptoms, and repeat scans over time show the lipoma to be without change in size and consistency.1