pneumococcal vaccination indications
- related: Infectious Disease ID
- tags: #literature #icu #id
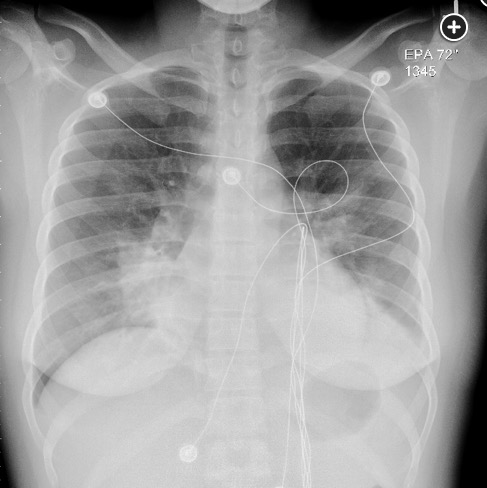
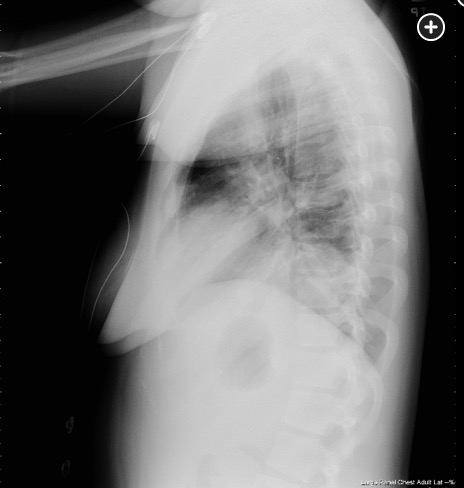
The underlying conditions for severe pneumococcal infection parallel the indications for pneumococcal vaccine: functional or anatomical asplenia, HIV infection, lymphoma (both Hodgkin and non-Hodgkin), and multiple myeloma. An additional risk factor for severe pneumococcal infection is alcohol use disorder. Analogous to herpes zoster infection (in which immunosuppression is a classic risk factor for the development of multidermatomal zoster), compromise of humoral immunity (as can occur with multiple myeloma and lymphoma) predisposes to the development of multilobar pneumococcal pneumonia. Given this patient’s severe clinical course with multilobar involvement, a search for an immunocompromising state would be prudent. Her age argues against multiple myeloma but in favor of lymphoma, which could result in a defect in her humoral immunity. The finding of intrathoracic lymphadenopathy, which was suspected based on the findings on her admission chest radiographs, would be consistent with such a diagnosis (choice A is correct).
Austrian triad, which is composed of pneumococcal pneumonia, meningitis, and endocarditis, was named after Dr. Robert Austrian, who in 1957 presented eight cases that were associated with aortic valve rupture (of which six patients died). With pneumococcal infection, the pathogenesis is generally that respiratory tract infection leads to seeding of the heart valves in those situations when endocarditis develops. There are no findings on physical examination suggesting endocarditis. This patient has no neurological signs or symptoms to suggest meningitis (choice B is incorrect).
There were no symptoms prior to her acute illness that suggested a histamine-mediated phenomenon as might occur with a carcinoid tumor, and there does not appear to be any evidence of volume loss in her lungs that might occur on the basis of an obstructing airway lesion with a secondary pneumonia (choice C is incorrect).
In reviews of severe pneumococcal community-acquired pneumonia admitted to the ICU, the stated mortality is 29%. Independent factors associated with early death were acknowledged to be age, altered mental status, multilobar pneumonia, shock, bacteremia, and inadequate empiric antibiotic therapy. Drug resistance did not have any significant impact on severity or mortality (choice D is incorrect).123456
A 28-year-old woman with no known medical conditions presents to the ED with a 3-day history of fever, productive cough, and increasing shortness of breath. Prior to the onset of this illness she had experienced no other symptoms or signs, and there is no relevant epidemiological history related to her illness. On exam, she is acutely ill but is oriented to time, place, and person. Her temperature is 39.2°C, with a BP of 96/78 mm Hg, pulse of 122/min, and respirations of 34/min. Chest exam reveals diffuse crackles with consolidation findings over left lung base posteriorly. The remainder of her exam is unrevealing. Room air blood gases are a pH of 7.56, PCO2 of 29 mm Hg, and PO2 of 54 mm Hg. Her chest radiographs are shown in Figure 1 and Figure 2. Blood cultures drawn at the time of presentation are positive in 12 h for Streptococcus pneumoniae. Tests for HIV and influenza are negative. Based on this clinical presentation, what is the most likely finding that would explain the underlying basis for this patient’s clinical presentation of bacteremic pneumococcal pneumonia?
Links to this note
Footnotes
-
Austrian R. Pneumococcal endocarditis, meningitis, and rupture of the aortic valve. AMA Arch Intern Med. 1957;99(4):539-544. PubMed ↩
-
Bhatty M, Pruett SB, Swiatlo E, et al. Alcohol abuse and Streptococcus pneumoniae infections: consideration of virulence factors and impaired immune responses. Alcohol. 2011;45(6):523-539. PubMed ↩
-
Bhatty M, Pruett SB, Swiatlo E, et al. Alcohol abuse and Streptococcus pneumoniae infections: consideration of virulence factors and impaired immune responses. Alcohol. 2011;45(6):523-539. PubMed ↩
-
Mongardon N, Max A, Bouglé A, et al. Epidemiology and outcome of severe pneumococcal pneumonia admitted to intensive care unit: a multicenter study. Crit Care. 2012;16(4):R155. PubMed ↩
-
Reyes LF, Restrepo MI, Hinojosa CA, et al. Severe pneumococcal pneumonia causes acute cardiac toxicity and subsequent cardiac remodeling. Am J Respir Crit Care Med. 2017;196(5):609-620. PubMed ↩