polycythemia vera
- related: Hematology, essential thrombocytosis
- erythrocytosis
- questions to ask
- smoking history
- hormonal therapy (testosterone increases Hgb)
- OSA hx
- renal/liver cancer
- burning pain in hands/feet
- itching
- fatigue
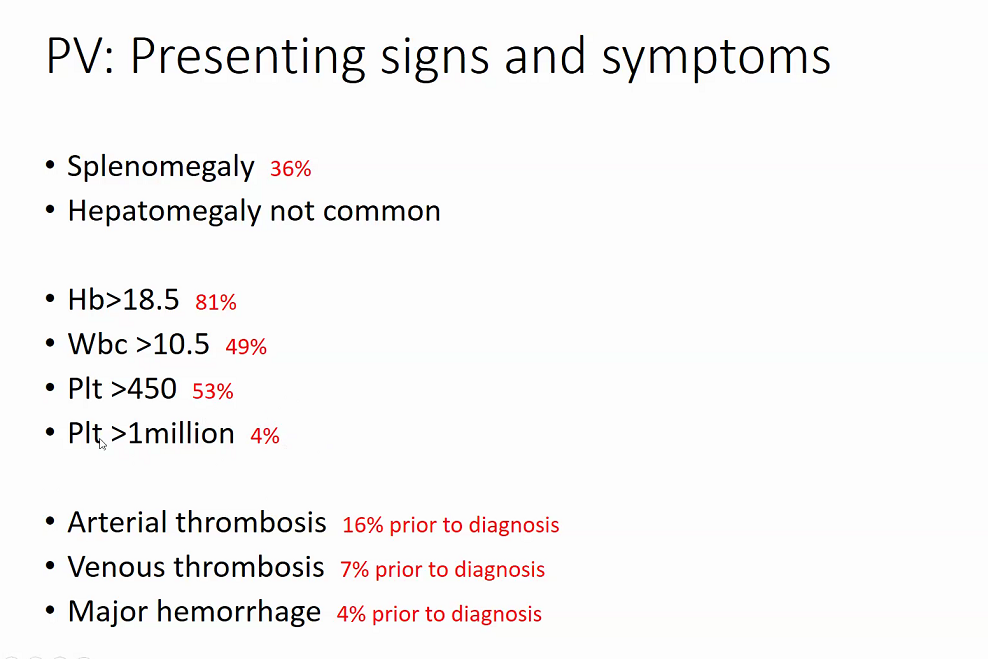
- physical exam findings
- facial plethora
- red extremities
- clubbing
- splenomegaly
- labs
- iron profile
- LDL
- uric acid
- EPO
- JAK2: both mutations
- can have both leukocytosis and thrombocytosis
Diagnosis
- initial bone marrow baseline
- eventually 1/5 will progress to myelofibrosis
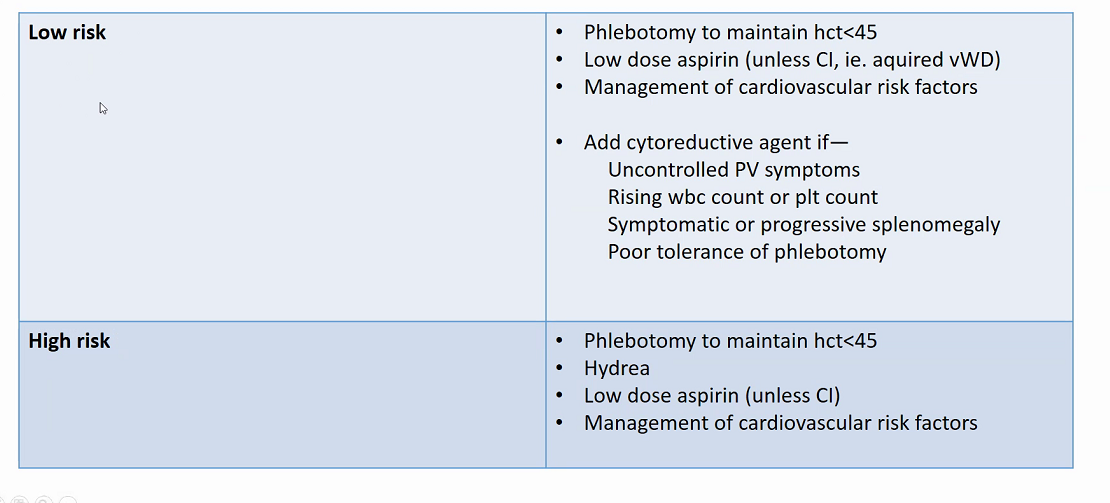
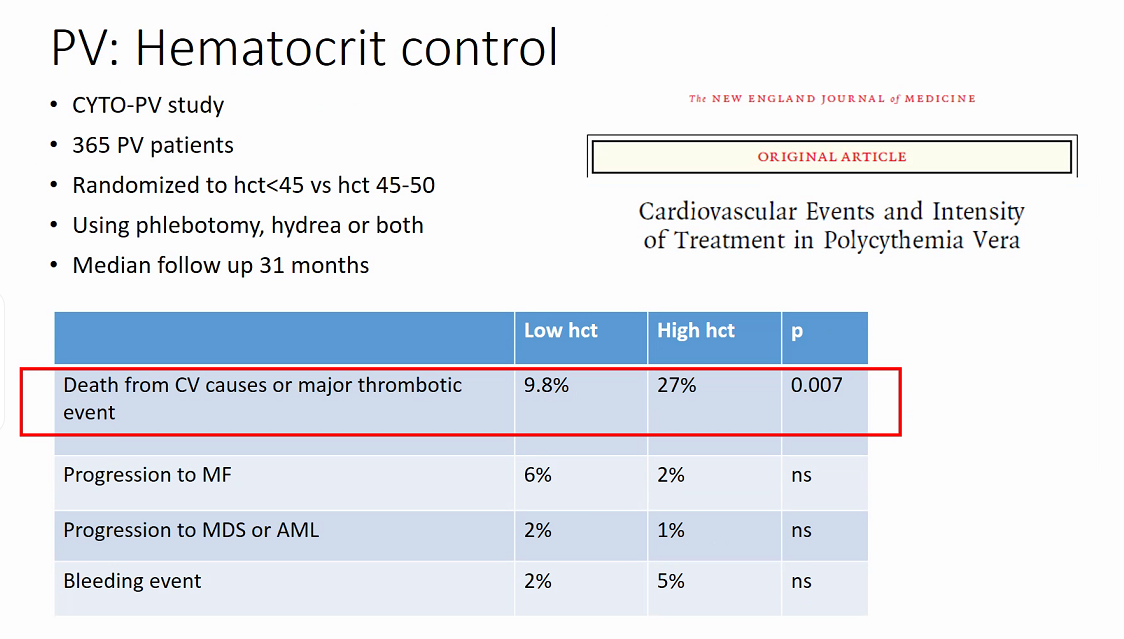
Treatment
- patients on testosterone therapy require hematocrit monitoring; testosterone supplementation should be decreased/discontinued if hematocrit levels are >54%.
- decrease thrombosis
- prevent bleed
- decrease sx
- no known agents to decrease progression to AML/MDS/MF
- low risk
- < 60
- no hx of thrombosis
- high risk
-
60
- hx of thrombosis
-
- Ruxolitinib
Prognosis
- untreated: 18 months
- treated: 13 years