schwannoma with pleural mass
- related: lung mass and cancer
- tags: #literature #pulmonology
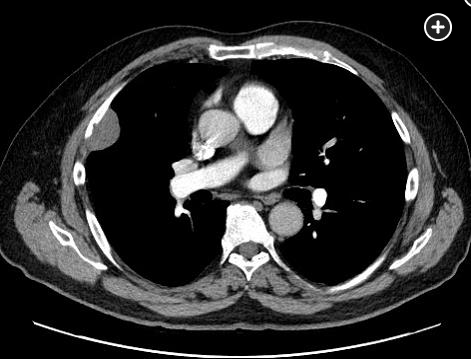
The combination of clinical and imaging features—incidental finding; no chest pain or chest wall tenderness; location of a smoothly marginated, well-circumscribed low-density mass near the neurovascular bundle of the rib with minor scalloping of the adjacent bone—makes Figure 2 the CT image most in keeping with a schwannoma diagnosis (choice A is correct). These lesions can show contrast enhancement, and a cystic component may be present that is best seen at MRI.
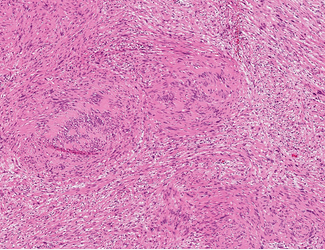
- The pathologic characteristics of this lesion demonstrate a characteristic somewhat cellular spindle cell area with areas of dense, eosinophilic cytoplasm (upper left and lower right corners) and other areas with more pale-staining cytoplasm (upper right and lower left corners). In the center region, there are rows of palisading spindle cells with an intervening anuclear zone, known as “Verocay bodies,” characteristic of these neoplasms. Hematoxylin and eosin stain (×60 magnification).

- Figure 3 Figure 3 shows a fatty lesion in the paraspinal region. This lesion had been present for 40 years and had been biopsied in the past. It was thought to be a lipoma (choice B is incorrect). Figure 4 shows a soft-tissue lesion of the chest wall, involving rib and associated with mediastinal adenopathy. Chest pain was part of the presentation, and a biopsy revealed a B-cell lymphoma (choice C is incorrect). Figure 5 shows a large mass that had developed rapidly. The mass involved the chest wall, with chest pain a prominent part of the presentation. Peripheral calcification and possible extension from the rib are seen. Results from biopsy of the mass showed an osteosarcoma (choice D is incorrect).
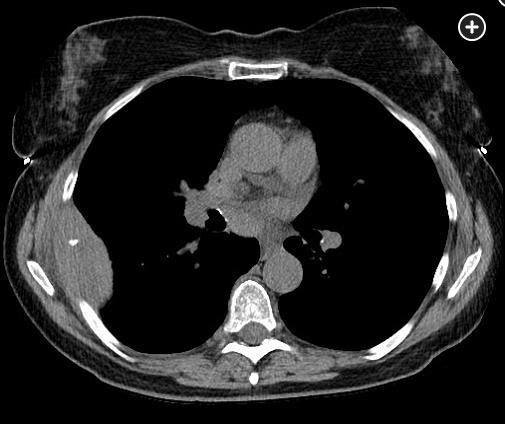
- Figure 4
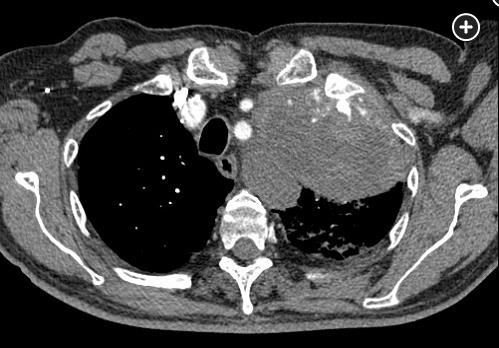
- Figure 5
It can be difficult to determine the cause of lesions that involve or are adjacent to the chest wall on the basis of their imaging appearance alone. Chest wall lesions can be classified at imaging by their attenuation as being fat, calcified, containing fluid, or being mostly soft tissue.
Lipomas are the most common benign fat-containing chest wall lesion. They are mostly adipose tissue surrounded by thin fibrous tissue, possibly with thin septa, and located in the deeper soft tissues. Up to one-third may contain foci of calcification. There are less common benign fat-containing lesions as well, such as spindle cell lipomas. Liposarcomas are the most common malignant fat-containing chest wall lesion. Imaging features that can help distinguish them from lipomas include septa greater than 2 mm in thickness, size larger than 10 cm, a lower percentage of the lesion that is fat, and nodular soft-tissue areas. Calcification can be seen, particularly when well differentiated.
Calcified lesions can arise from bone or occur within soft tissue. The most common benign lesion involving bone is fibrous dysplasia, which occurs developmentally when fibrous stroma replaces normal marrow and bone, often in the lateral or posterior aspect of the ribs. Osteochondromas are aberrant growth of bone tissue, often at the costochondral junction. Soft-tissue calcification can occur owing to end-stage renal disease or chronic inflammatory conditions. Myositis ossificans, characteristically peripheral calcification of a soft-tissue lesion, occurs in muscle after trauma. Chondrosarcoma and osteosarcoma are the most common malignant calcified chest wall lesions. Osteosarcomas have a denser, central cloudy pattern of ossification, whereas calcification is more peripheral in chondrosarcoma. Myeloma leads to expansile lytic bone lesions.
Benign soft-tissue lesions include elastofibroma dorsi, often manifesting as bilateral well-circumscribed masses with linear areas of interspersed fat (lasagna sign). Hemangiomas may have phleboliths, areas of macroscopic fat, and gradual enhancement after contrast administration. Nerve sheath tumors, most commonly schwannomas (adjacent to nerves) and neurofibromas (inseparable from nerves) usually arise from intercostal nerves and can extend into the neural foramina. Malignant peripheral nerve sheath tumors grow faster and to larger sizes and can lead to osseous destruction and distant metastases. Lymphoma involving the chest wall is often a result of direct invasion, although it can be seen as part of widely disseminated Hodgkin disease or diffuse large B-cell lymphoma. The most common primary malignant soft-tissue lesion of the chest wall is pleomorphic sarcoma.
Fluid-containing lesions include lymphatic malformations that can infiltrate extensively. Hematomas appear as a hyperattenuating collection. A layering, hematocrit-like appearance may be seen at MRI. Chest wall abscesses and extension of infection into the chest wall from an intrathoracic source can also be seen.1