second primary vs separate tumor nodule
- related: lung mass and cancer
- tags: #literature #pulmonology
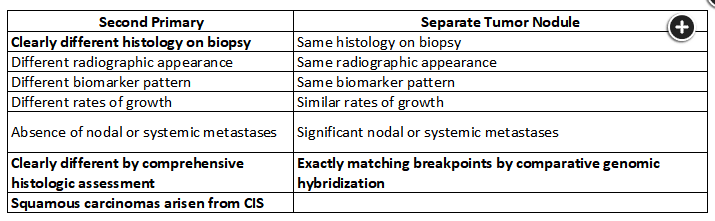
Distinguishing second primary lung cancers from a single lung cancer with separate tumor nodules. Bold represents an absolute indication. No bolding represents suggestive indicators.1
Distinguishing among these four patterns of multiple pulmonary sites of lung cancer assists with assigning the stage and determining optimal treatment. Separate tumor nodules are staged T3 if they are in the same lobe, T4 if in different lobes but in the same lung, and M1a if in the other lung. A single N and M is assigned and treatment is based on the overall stage. When a second primary cancer is present, each tumor receives its own T (tumor), N (lymph node), and M (metastases) stage with individual treatment plans. Staging of multifocal lung adenocarcinoma with ground glass and/or lepidic features includes assigning the T stage according to the highest T lesion with a ”#” or “m” (indicating multiplicity) and a single N and M for all lesions. Treatment is directed at the largest or most aggressively evolving of the lesions. Pneumonic type adenocarcinomas are staged based on their size if a single site, T3 if more than one site in the same lobe, T4 if in an ipsilateral lobe, and M1a if in the contralateral lung. A single N and M is assigned and treatment is based on the stage.
It can be difficult to determine whether more than one tumor nodule represents separate primary cancers or intrapulmonary metastases. Comprehensive histologic and molecular characterization of the tumors is required to make this determination. This information was not provided in the case described (choice A is correct; choices B, C, and D are incorrect).
It is common for multiple lung nodules to be noted in an individual with lung cancer. Often these are very small solid nodules that require only imaging monitoring over time. When multiple pulmonary sites of cancer are present, they fall into one of four patterns: separate primary lung cancers, separate tumor nodules of the same cancer, multiple tumors with prominent ground-glass features on imaging or lepidic histologic features, or a diffuse pneumonic pattern.
Distinguishing second primary cancers from separate tumor nodules of the same cancer can be very difficult. Clinical and pathologic criteria are used to help with the distinction. Tumors of clearly different histology or histologic subtype are considered separate primary cancers, while those of the same histology with exactly matching breakpoints by comparative genomic hybridization may be considered to be from the same cancer. Features that favor separate tumors include differences in their imaging appearance, different behavior (eg, rate of growth), absence of regional spread (ie, nodal involvement), and the presence of different molecular biomarker patterns.
It has become more common to find patients with multiple tumors with a prominent ground-glass component. These tumors tend to behave indolently, with excellent survival and a low rate of regional or distant spread. Each tumor site usually behaves independently. This behavior has shaped thoughts about staging and treatment of these tumors. Diffuse pneumonic-type presentations are associated with more aggressive disease and poorer prognosis, though they are still less likely to spread to nodal or distant sites. They are usually invasive mucinous adenocarcinomas.
Staging of multiple tumor nodules deemed to be due to second primary lung cancers is based on the understanding that they are considered unrelated tumors. Separate TNM classifications are assigned to each tumor. Separate tumor nodules of the same cancer are staged as one cancer. T3 is applied when the tumors are in the same lobe, T4 when in separate lobes of the same lung, and M1a when in separate lungs. Multifocal ground-glass/lepidic-predominant nodules are given one overall stage but are considered separate tumors. The T is based on the highest T lesion with (#/m) indicating multiplicity. A single N and M are applied. Pneumonic-type adenocarcinomas are staged like other primary lung cancers (a single T, N, and M, with the T based on size and location of the primary and/or separate tumor nodules).
The tumor nodules in the patient in this question were found to have different histologic subtypes, one predominantly micropapillary and the other papillary. Driver mutations were not identified in the micropapillary adenocarcinoma and PD-L1 expression was 0%, whereas a K-ras mutation was present in the papillary adenocarcinoma and PD-L1 expression was 90%. These tumors were managed as separate primaries and staged as T1bN0M0 (stage IA2) and T1aN0M0 (stage IA1).