systolic anterior motion SAM mitral valve in sepsis ultrasound and management
- related: Cardiology and Hemodynamics
- tags: #literature #cardiology
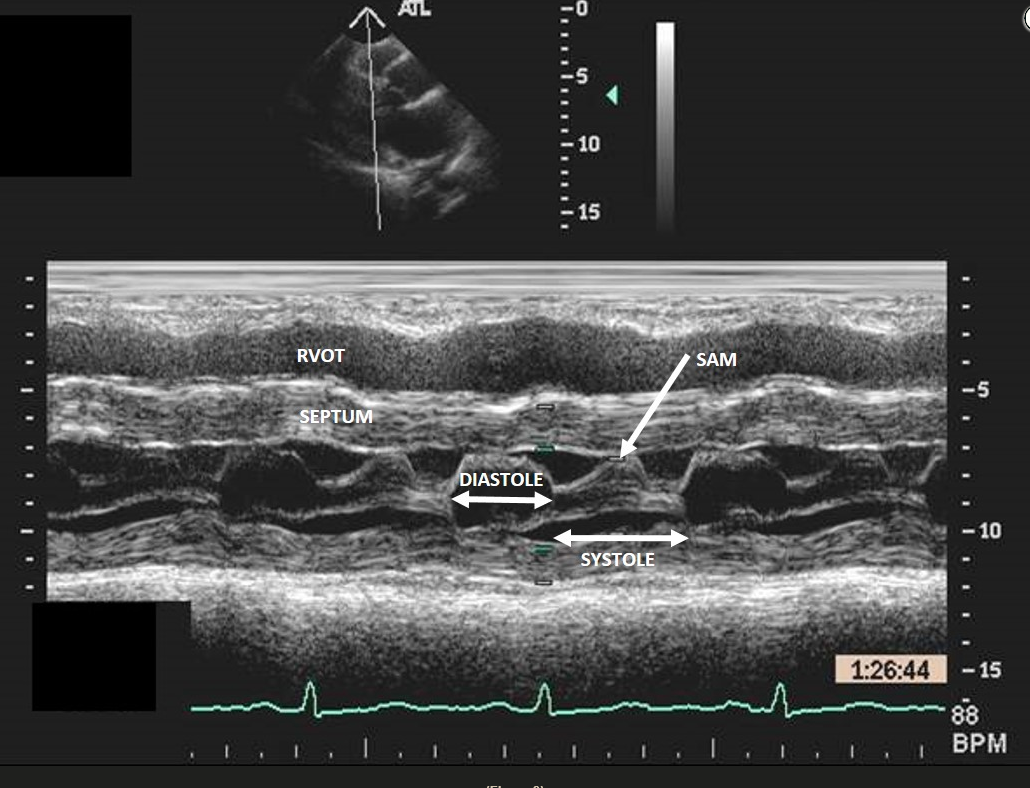
Early septic shock is often characterized by hypovolemia, reduced left ventricular afterload, and increased inotropy, conditions that favor intraventricular flow obstruction (IVO). Left ventricular hypertrophy may contribute, especially in patients with hypertrophic obstructive cardiomyopathy (HOCM), but IVO is seen in roughly 20% of all patients in early sepsis. Dynamic obstruction is usually localized to the left ventricular outflow tract (LVOT) and due to systolic anterior motion of the mitral valve as flow acceleration tends to draw the anterior leaflet into the LVOT (Bernoulli effect). IVO is sometimes seen in the midventricle, particularly in association with takotsubo cardiomyopathy. In this case, M-mode imaging across the mitral valve shows normal valve opening during diastole but abnormal anterior motion of the anterior mitral leaflet during systole, or systolic anterior motion (SAM) (Figure 3). For comparison, both mitral leaflets should remain opposed throughout systole (Figure 2, arrow). The case patient also has HOCM (interventricular septum measures 1.9 cm). Other echocardiographic findings of SAM include turbulent flow visualized as a mosaic pattern on color Doppler imaging; early systolic closure of the aortic valve and fluttering of the aortic valve leaflets; and high, late-peaking flow seen on continuous-wave Doppler imaging through the LVOT.
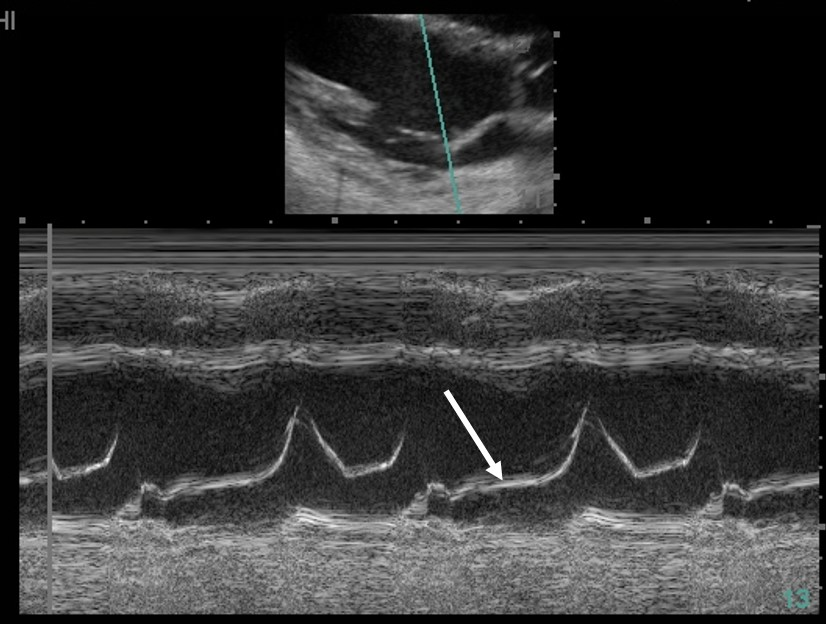
Normal M-mode of mitral valve showing the expected position of the anterior mitral leaflet during systole (arrow).
Dynamic IVO is important to recognize because of the therapeutic implications. Fluid loading is the first step. When a vasoconstrictor is used, drugs like vasopressin and phenylephrine are preferred due to the absence of inotropy, but these are given only when fluids are incompletely effective or contraindicated. Treatments that reduce afterload or enhance contractility are generally avoided.
Goal-directed echocardiography (GDE) is often helpful in the differential diagnosis of shock and may serve to guide therapy. GDE allows the intensivist to assess right and left ventricular function, valvular abnormalities, and pericardial disease and to gain clues to fluid responsiveness. By additionally imaging the lungs, pleurae, abdomen, and retroperitoneum, other clues to the origin of shock can be identified.1234
Links to this note
Footnotes
-
Chauvet JL, El-Dash S, Delastre O, et al. Early dynamic left intraventricular obstruction is associated with hypovolemia and high mortality in septic shock patients. Crit Care. 2015;19:262. PubMed ↩
-
Ghadri JR, Wittstein IS, Prasad A, et al. International expert consensus document on takotsubo syndrome (part II): diagnostic workup, outcome, and management. Eur Heart J. 2018;39(22):2047-2062. PubMed ↩
-
Schmidt GA, Koenig S, Mayo PH. Shock: ultrasound to guide diagnosis and therapy. Chest. 2012;142(4):1042-1048. PubMed ↩