think WPW in afib with wide QRS
- related: cardiac arrythmia
- tags: #literature #icu #cardiology
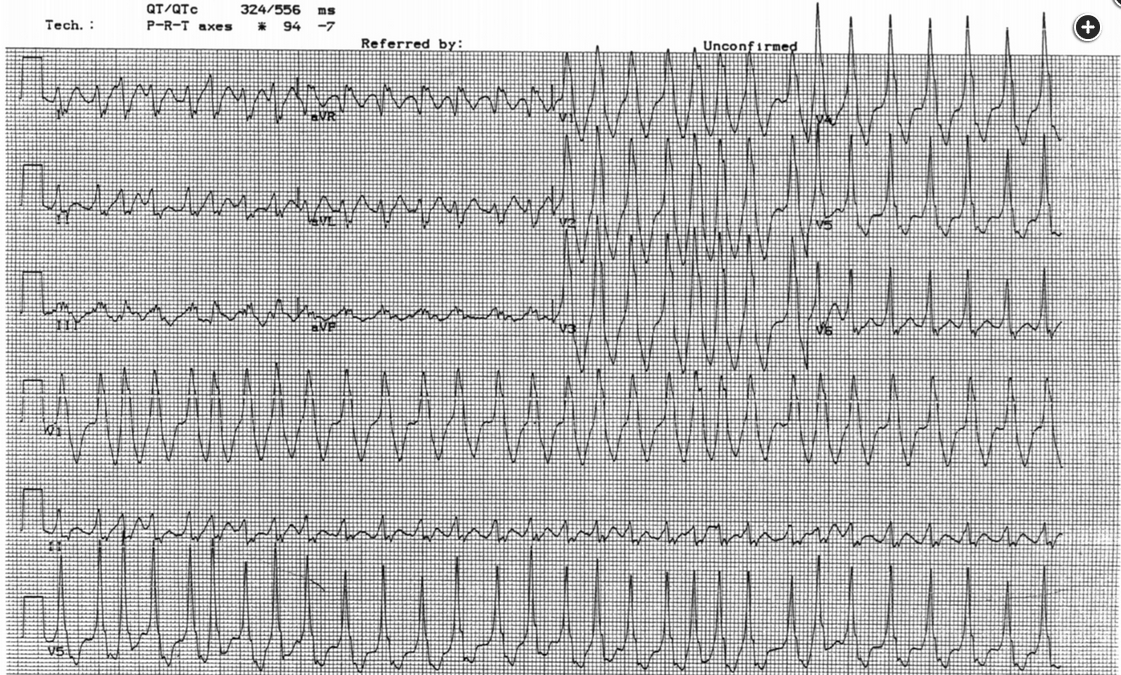
The rhythm is atrial fibrillation—it is irregularly irregular without discernible P waves. Some of the intervals are very short—the interval between the second and third beat is about 220 milliseconds; if sustained, this would correspond to a heart rate of 273/min. The QRS complex is wide in some beats, narrower in others, and in fact, differs from beat to beat. This combination of features makes the diagnosis of Wolff-Parkinson-White (WPW) syndrome with atrial fibrillation.
Although, classically, WPW is diagnosed by the presence of a short PR interval and a delta wave in sinus rhythm, it is important to be able to make the diagnosis of WPW with atrial fibrillation when presented with an ECG such as this one. The reason is that WPW is characterized by the presence of dual pathways, one conducting through the atrioventricular (AV) node and the other a bypass tract that inserts directly into the His-Purkinje system and bypasses the AV node. In atrial fibrillation, the ventricular rate is determined by competition between impulses that go through the AV node and those that go down the bypass tract; the AV node has limited conduction (that is, type 1 [Wenckebach] second-degree AV block is a normal response to atrial rates that are fast enough in order to protect the ventricles), but the bypass tract does not. As such, in WPW with atrial fibrillation, drugs that slow AV nodal conduction increase the number of impulses that go down through the bypass tract and actually increase ventricular rate in this setting. Only drugs that slow conduction down the bypass tract are indicated.
Procainamide slows conduction down bypass tracts in WPW. Although some of the complexes are wide, this is not ventricular tachycardia, which can be slightly irregular but not to this extent, and which would have the same QRS width with every beat.
Lidocaine is effective only in ventricular tachycardia.
Adenosine causes AV nodal blockade and so, as above, would increase the ventricular rate in this setting. Although that increase would likely be transient, there have been case reports of adenosine precipitating ventricular fibrillation in WPW with atrial fibrillation.
Esmolol also causes AV nodal blockade.1234
This patient has developed an acute tachyarrhythmia. At first glance, the QRS complex appears wide. However, closer inspection shows that the tachyarrhythmia is irregularly irregular.
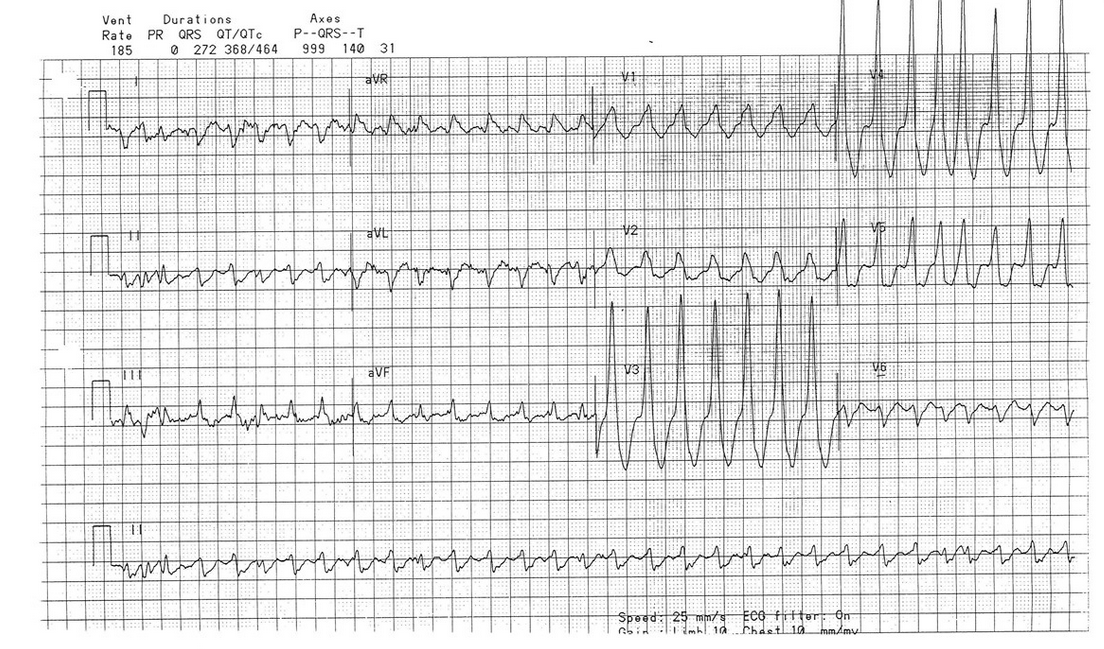
Furthermore, the widths of the QRS are also irregular and vary between beats (best seen in the six-lead rhythm strip or lead V4 of the 12-lead ECG).

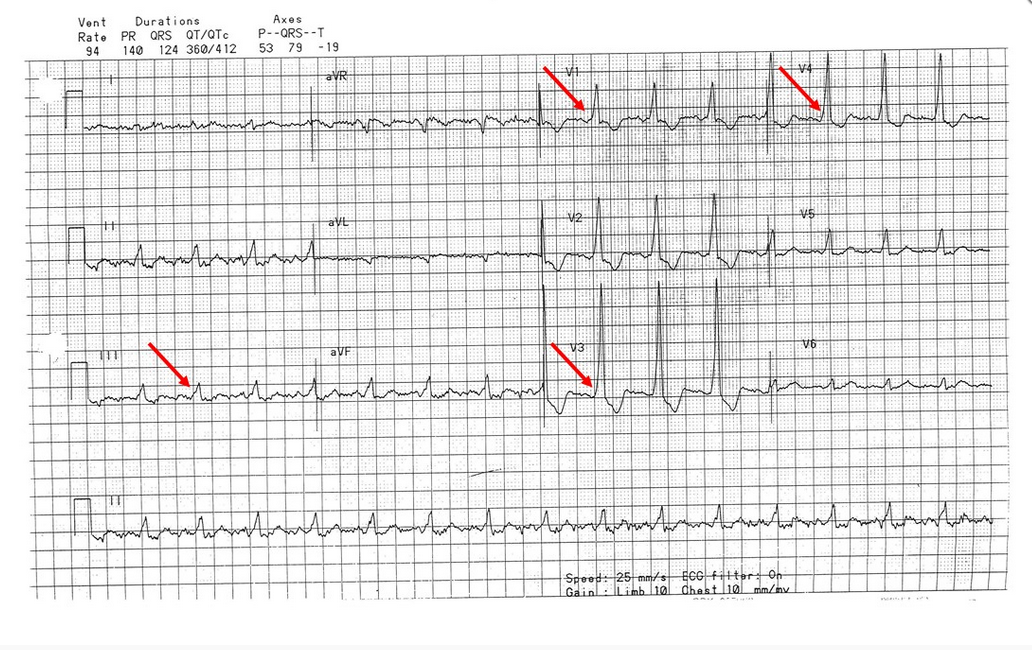
These three criteria, namely wide complex tachyarrhythmia, irregularly irregular rhythm, and varying widths of the QRS complexes, should prompt consideration of preexcited atrial fibrillation or atrial fibrillation in a patient with an accessory conduction pathway. This is also called preexcitation syndrome or Wolff-Parkinson-White syndrome. Patients with preexcitation syndrome have an accessory conduction pathway that directly connects the atria with the ventricles and bypasses the atrioventricular (AV) node. If conduction occurs through this accessory pathway, the ventricles are activated sooner than when the impulse travels through the AV node. This activation, which is referred to as preexcitation, results in the classic ECG findings of shortened PR interval and widened QRS complex due to a delta wave (red arrows in Figure 3).
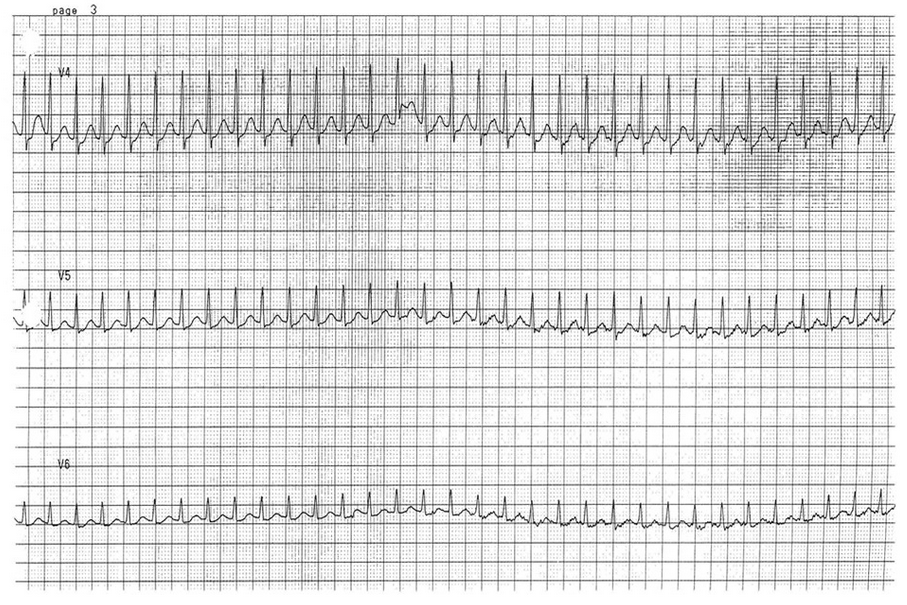
While radiofrequency ablation is the treatment of choice, and curative, oftentimes patients with preexcitation pathways present with tachyarrhythmias. They can develop AV nodal reentry tachycardias when conduction occurs either down the AV node, into the ventricle and back up through the accessory pathway into the atria or through the accessory pathway into the ventricle and retrograde up through the AV node back into the atria. These tachyarrhythmias are narrow complex and regular (Figure 4).
When patients with preexcitation pathways develop atrial fibrillation or atrial flutter, conduction occurs through both the accessory pathway and the AV node. Since most accessory pathways have a shorter refractory period than the AV node, this can result in really rapid ventricular rates. Patients who demonstrate signs or symptoms of hemodynamic instability, such as hypotension, chest pain, or confusion, should undergo urgent electrical cardioversion. Patients without hemodynamic instability can be treated medically.
The goal of medical treatment is to both slow conduction through the accessory pathway and convert the atrial fibrillation or flutter back to sinus rhythm. Preferred agents include ibutilide and procainamide (choice D is correct). Ibutilide is a Class III antiarrhythmic drug that prolongs refractoriness of both the AV node and accessory pathway and acutely terminates atrial fibrillation or flutter. Procainamide is a Class Ia antiarrhythmic that increases refractoriness of atrial and ventricular myocardium without any AV nodal-blocking effect. It can also be effective for acute termination of preexcited atrial fibrillation, and even when it fails to terminate the atrial fibrillation, it usually slows the ventricular rate due to decreased conduction and increased refractoriness in the accessory pathway.
AV nodal-blocking agents normally used to control ventricular rate in patients with atrial fibrillation are contraindicated in patients with preexcitation atrial fibrillation. Blocking the AV node risks increasing conduction of atrial impulses to the ventricle through the accessory pathway, resulting in an increased ventricular rate and potentially exacerbating hemodynamic instability. Digoxin blocks AV nodal conduction and has an unpredictable effect on the accessory pathway refractoriness (choice A is incorrect). Adenosine selectively blocks the AV nodal pathway and may precipitate ventricular fibrillation (choice B is incorrect). Verapamil is potentially the most dangerous AV nodal-blocking agent in preexcitation atrial fibrillation as it lengthens AV nodal refractoriness, without an effect on the accessory pathway, and also reduces myocardial contractility and systemic vascular resistance, which increases sympathetic tone and further shortens the refractoriness of the accessory pathway (choice C is incorrect). Although amiodarone may slow conduction through the accessory pathway with chronic administration, it does not slow accessory pathway conduction with acute IV administration, and its β-blocking properties make it a primarily AV nodal-blocking agent in the acute setting, making it a nonpreferred agent in preexcited atrial fibrillation.567
A 28-year-old man with stage IIC testicular seminoma is being treated with bleomycin, etoposide, and cisplatin chemotherapy. During his third cycle, a rapid response is called to his room for tachycardia. Vital signs include a temperature of 37°C, heart rate of 180/min, BP of 111/72 mm Hg, and respiratory rate of 22/min. A 12-lead ECG (Figure 1) and six-lead rhythm strip (Figure 2) are obtained.
Which of the following agents should be given to manage his tachycardia?
Links to this note
Footnotes
-
Osmancik PP, Stros P, Herman D. In-hospital arrhythmias in patients with acute myocardial infarction - the relation to the reperfusion strategy and their prognostic impact. Acute Card Care. 2008;10(1):15-25. PubMed ↩
-
Redfearn DP, Krahn AD, Skanes AC, et al. Use of medications in Wolff-Parkinson-White syndrome. Expert Opin Pharmacother. 2005;6(6):955-963. PubMed ↩
-
Wolff L, Parkinson J, White PD. Bundle-branch block with short P-R interval in healthy young people prone to paroxysmal tachycardia. 1930. Ann Noninvasive Electrocardiol. 2006;11(4):340-353. PubMed ↩
-
Glatter KA, Dorostkar PC, Yang Y, et al. Electrophysiological effects of ibutilide in patients with accessory pathways. Circulation. 2001;104(16):1933-1939. PubMed ↩
-
January CT, Wann LS, Alpert JS, et al; ACC/AHA Task Force Members. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation. 2014;130(23):2071-2104. PubMed ↩
-
Page RL, Joglar JA, Caldwell MA, et al; Evidence Review Committee Chair. 2015 ACC/AHA/HRS guideline for the management of adult patients with supraventricular tachycardia: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation. 2016;133(14):e506-e574. PubMed ↩