thymoma can have drop metastases to pleura
- related: anterior mediastinal mass includes teratoma, thymoma, thyroid, lymphoma
- tags: #literature #pulmonology
- anterior mediastinal mass
- drop metastases to lower lung pleura
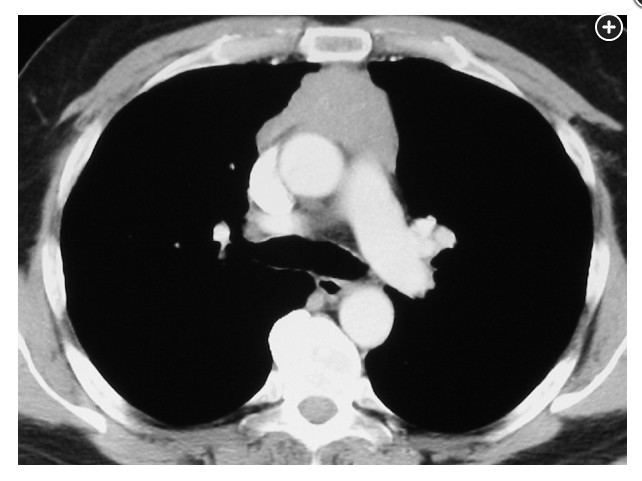
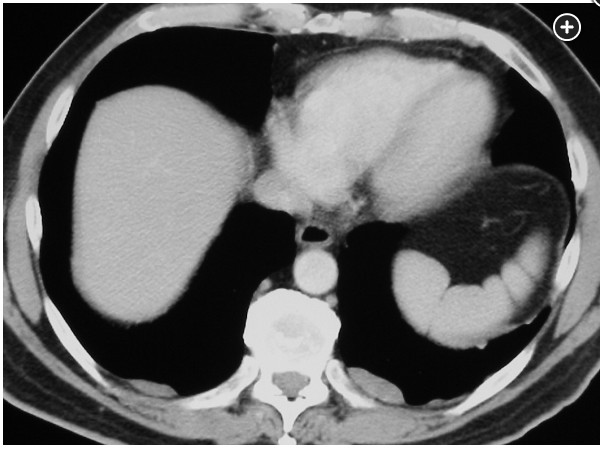
This patient has a soft-tissue lobulated mass in the anterior mediastinum and bilateral pleural-based masses (Figure 1, Figure 2). In the absence of radiographic abnormalities suggesting alternative diagnoses, the most likely diagnosis is invasive thymoma with “drop metastases” to the pleura (choice B is correct). Thymoma is the most common neoplasm of the anterior mediastinum, with a peak incidence from age 40 to age 60. “Malignancy” is defined by invasive behavior rather than by histologic features. Thymoma rarely metastasizes through the bloodstream or lymphatics; rather, it spreads locally or seeds the pleural or pericardial surfaces, as in this case. It may also spread through the diaphragm into the abdomen. Thymoma can be classified as encapsulated, invasive (invading into and beyond the capsule), and metastasizing, with pleural and pulmonary parenchymal seeding but no extrathoracic involvement. In this case, the tumor invaded into and through the mediastinal pleura, later leading to “drop metastases” with migration and proliferation of malignant cells in the lower recesses of the pleura. When thymoma invades through the capsule, it may proceed to invade local mediastinal structures and vessels, and may cause airway and superior vena cava obstruction. Extensive chest wall invasion may encase the lung and resemble malignant mesothelioma. Tissue sampling of one of the pleural masses using fine-needle aspiration would provide both histologic diagnosis and staging. Treatment of invasive and metastatic thymoma includes surgical resection, radiation, and chemotherapy.
Although TB can involve mediastinal lymph nodes and pleura, especially in patients with immune deficiencies, tuberculous lymph nodes would probably have a wider distribution than a single mediastinal mass, show necrosis (not the homogeneous density that this case exhibits), and be associated with systemic symptoms. For these reasons, TB is unlikely (choice D is incorrect). Hodgkin lymphoma usually involves the anterior mediastinum and the pleura, but most patients with this disease also have involvement of other lymph nodes; in this case, the coincidental finding of pleural based-masses also makes that diagnosis unlikely (choice A is incorrect). Mediastinal involvement with non-Hodgkin lymphoma is usually in the middle mediastinum, and extrathoracic lymph nodes are involved in the great majority of cases. Small-cell carcinoma may also present with prominent mediastinal lymphadenopathy and pleural involvement, but the large anterior mediastinal mass and pleural masses in the absence of a discernible lung mass and pleural effusion makes that diagnosis unlikely (choice C is incorrect).1