trauma resuscitation mtp
- related: ICU intensive care unit
- tags:
stage 1
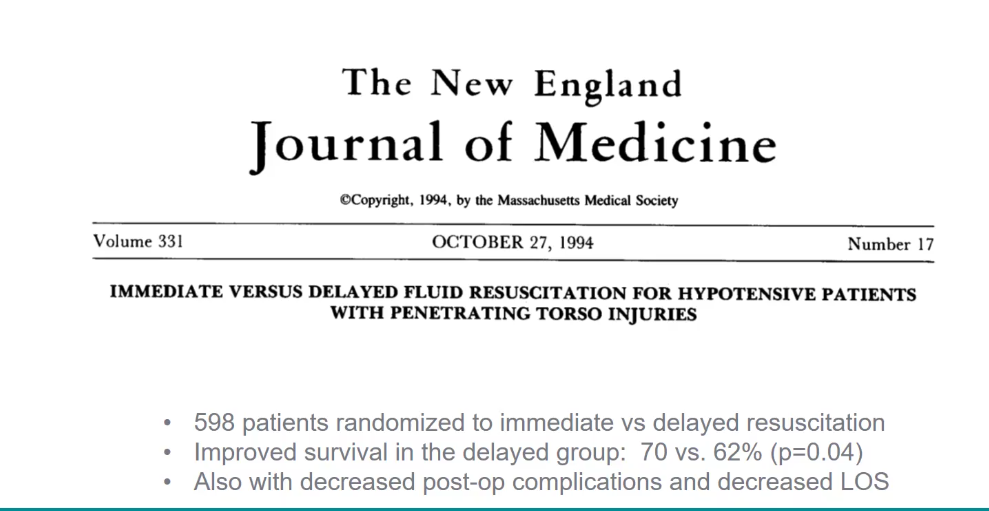
Permissive hypotension
- permissive hypotension is ok for penetrative (not blunt, normotension) torso trauma in ED: 70/palpable is ok. NNT 12
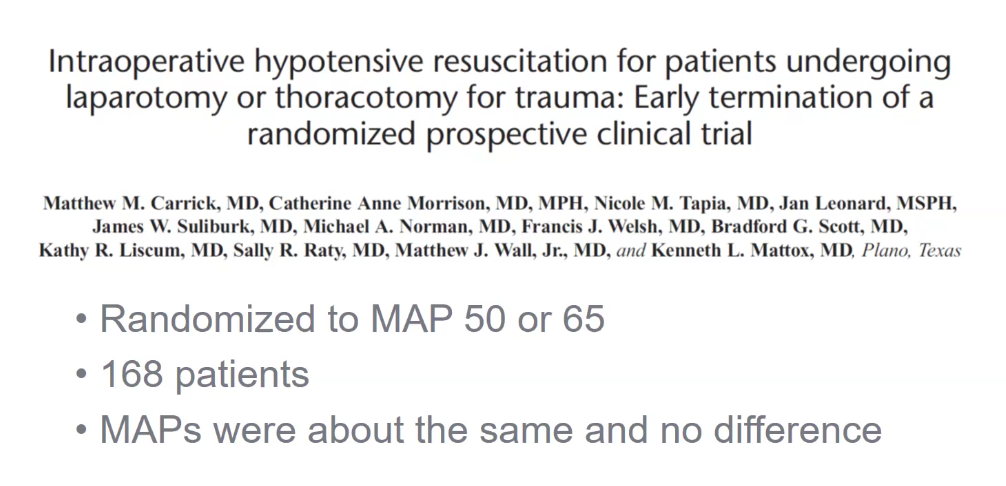
- permissive hypotension in OR with MAP 50 terminated earlier due to cannot get MAP separated between 2 groups
MTP
- MTP: original def 10u/24hrs
-
3u prbc in 1 hr
- in the past: BP, UOP
- today: prevent coagulopathy, AKI, ARDS, consequence of reperfusion
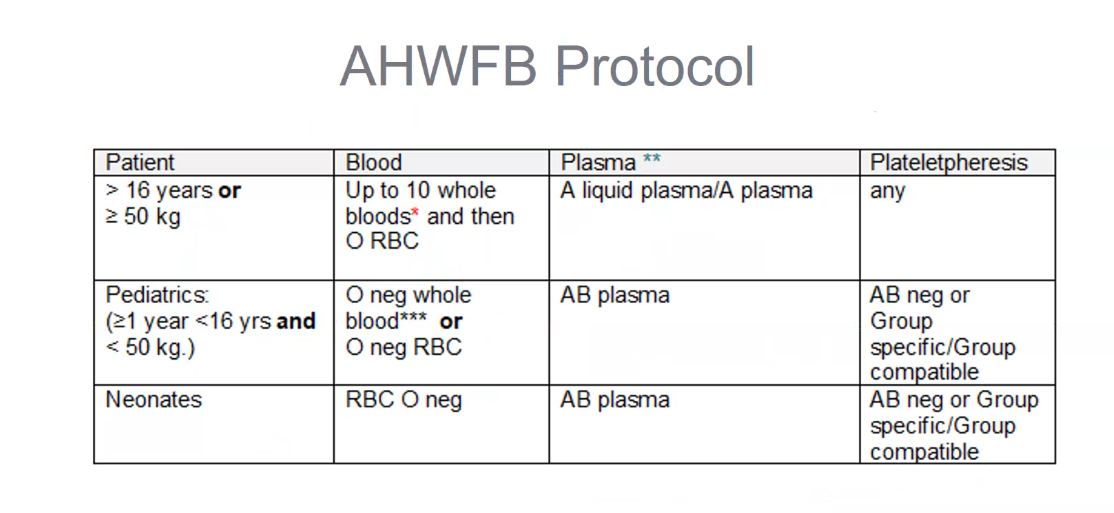
- new: RH+ whole blood for pregnant women as well
- leukocyte reduced
- low titer O blood: low anti A / B levels
- whole blood: 500 cc
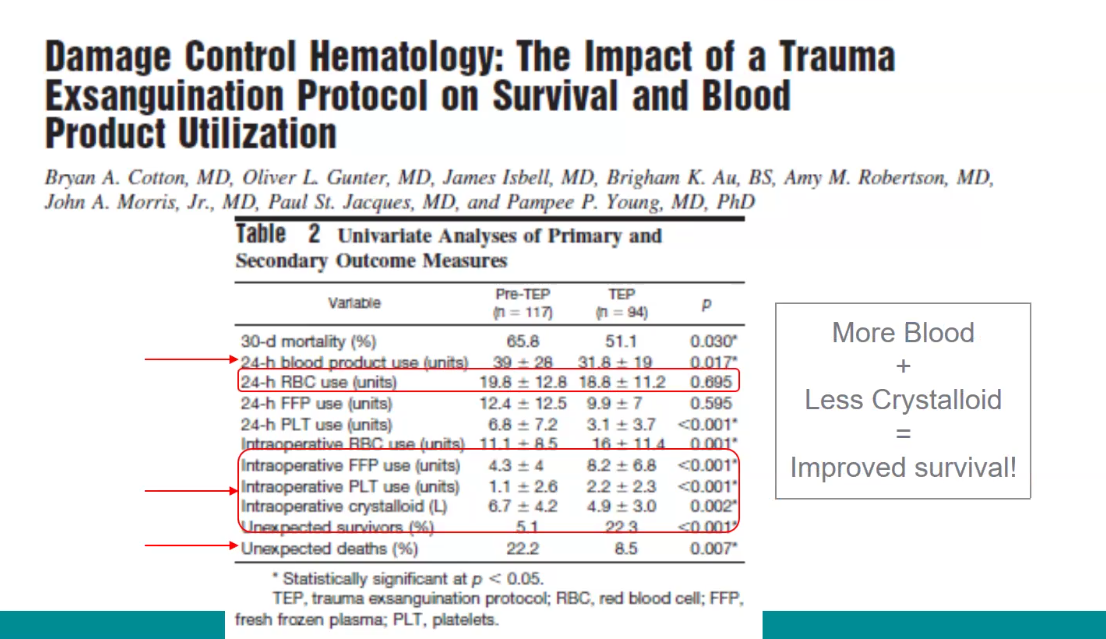
- 24h consumption less
- uses more upfront
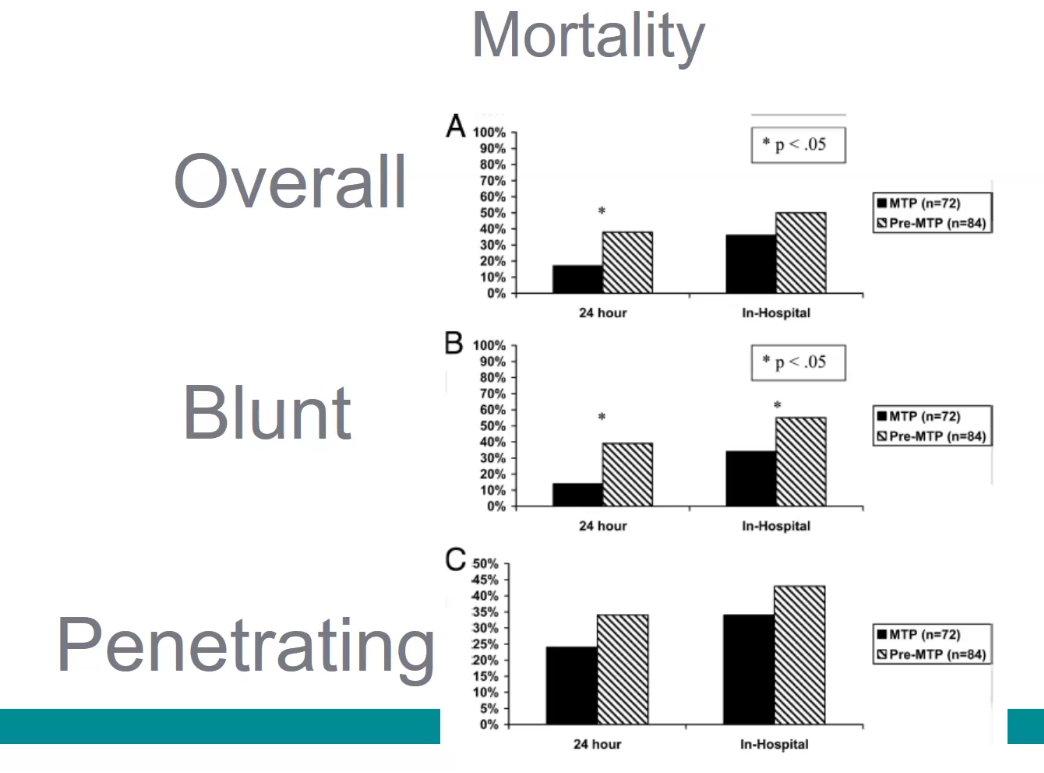
- blunt/penetrating trauma are very different
Stage 2
plasma and platelet
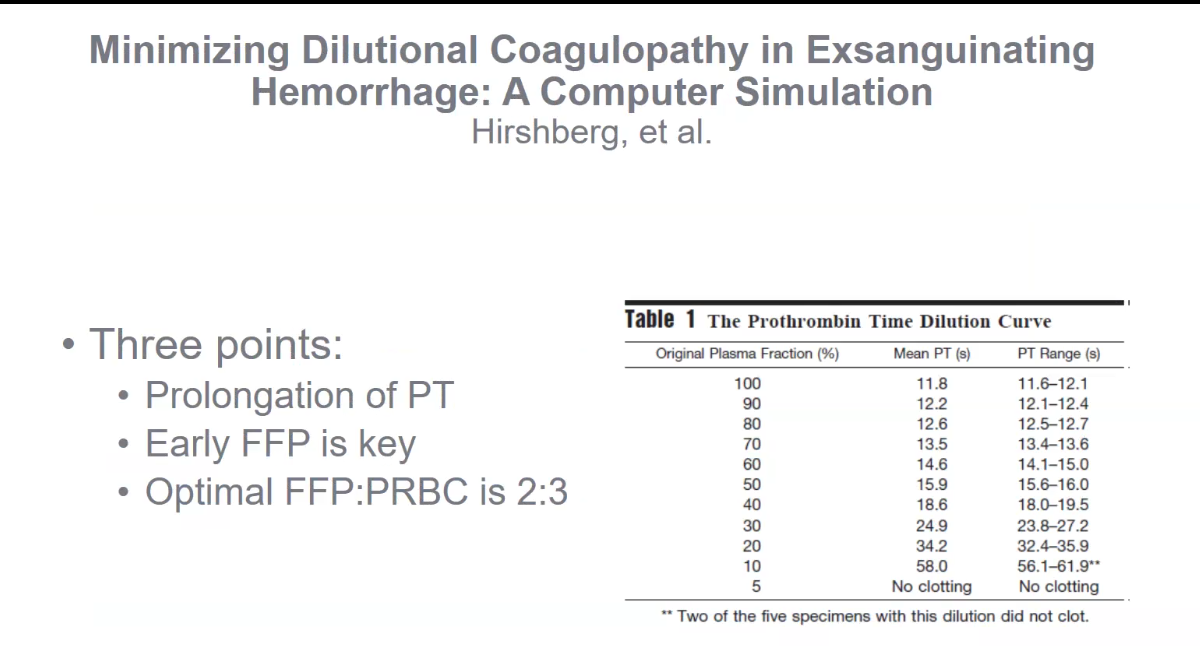
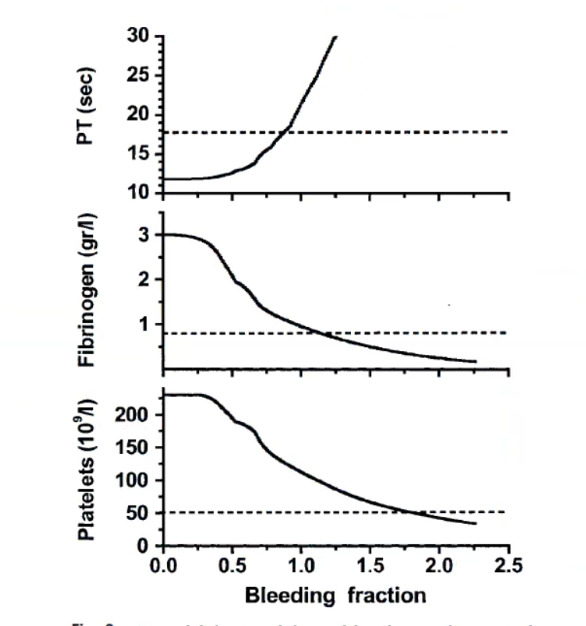
- bleeding fraction: how much original blood left
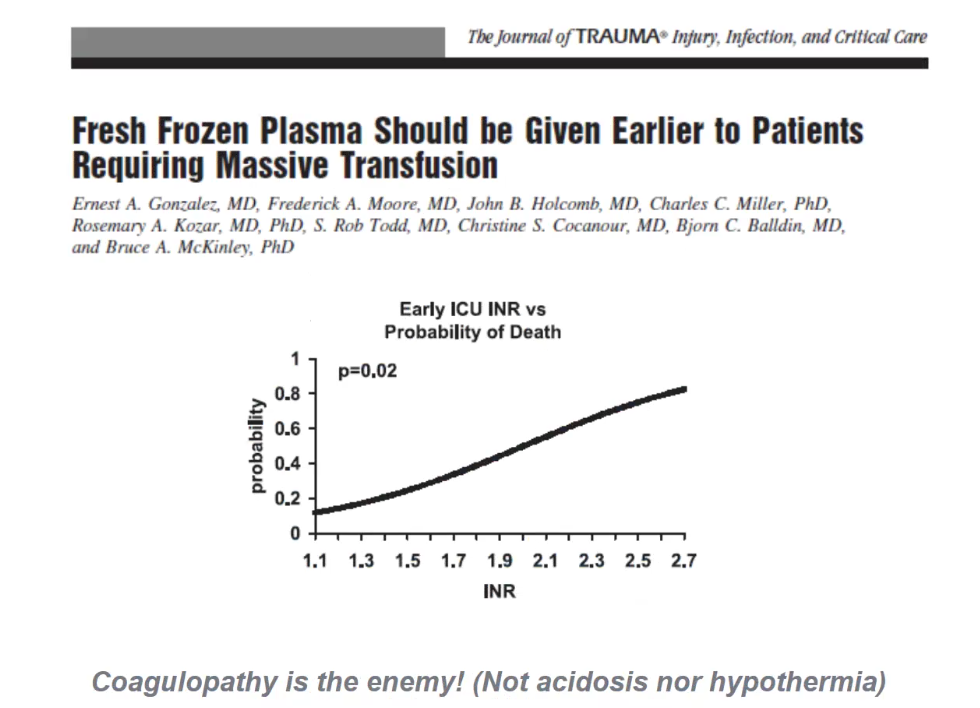
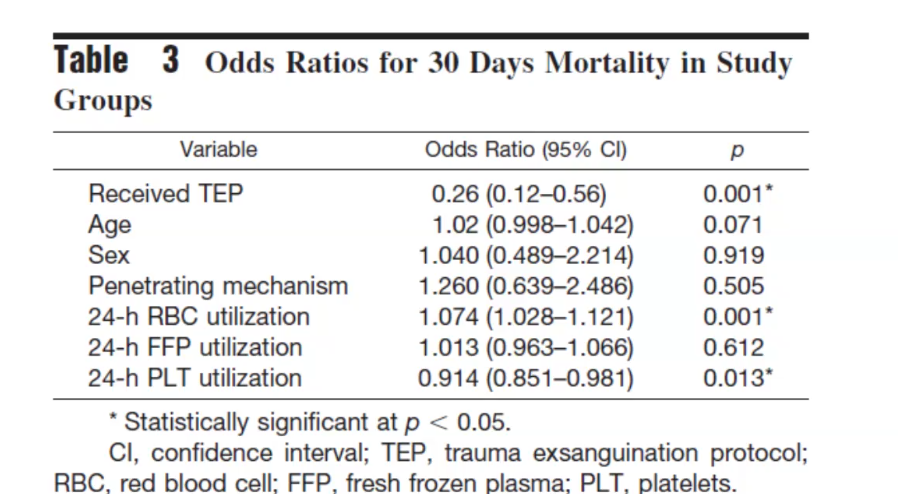
- higher INR = higher mortality. Lineaer relationship
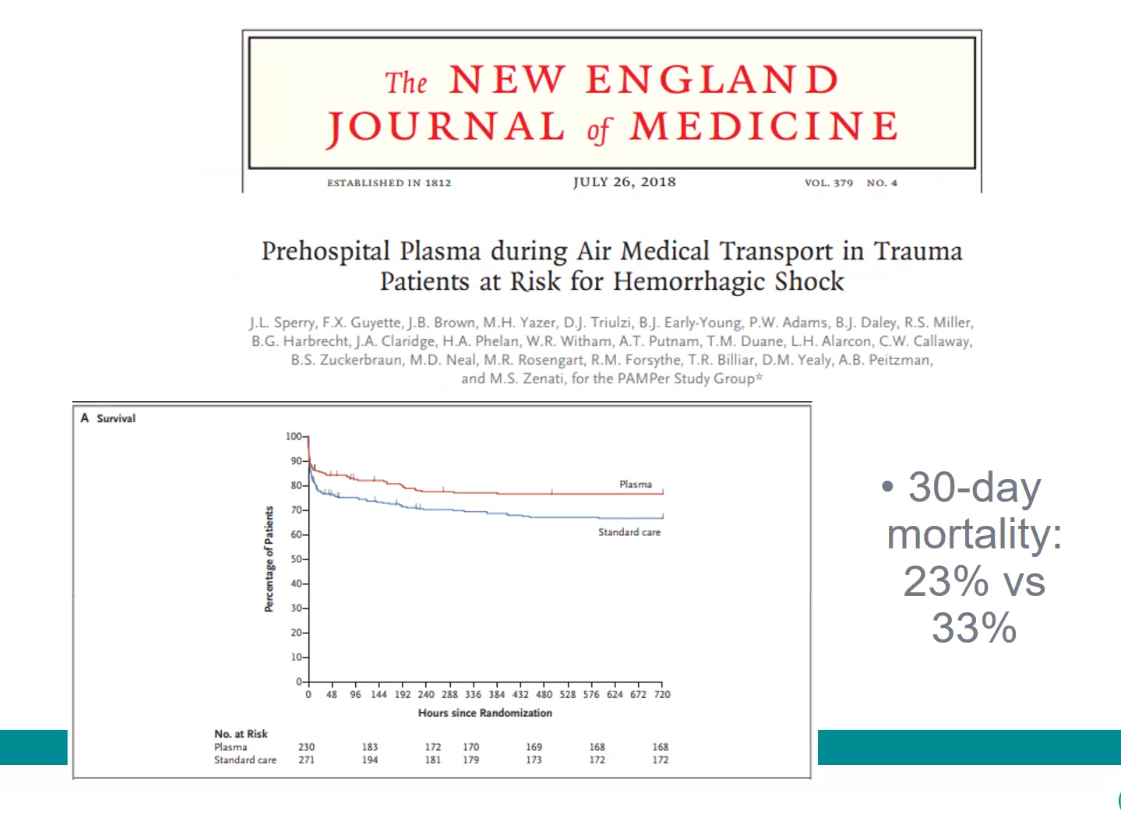
- big study
- balanced blood products in first 6 hours leads to best outcome. TEG can be used after 6 hrs
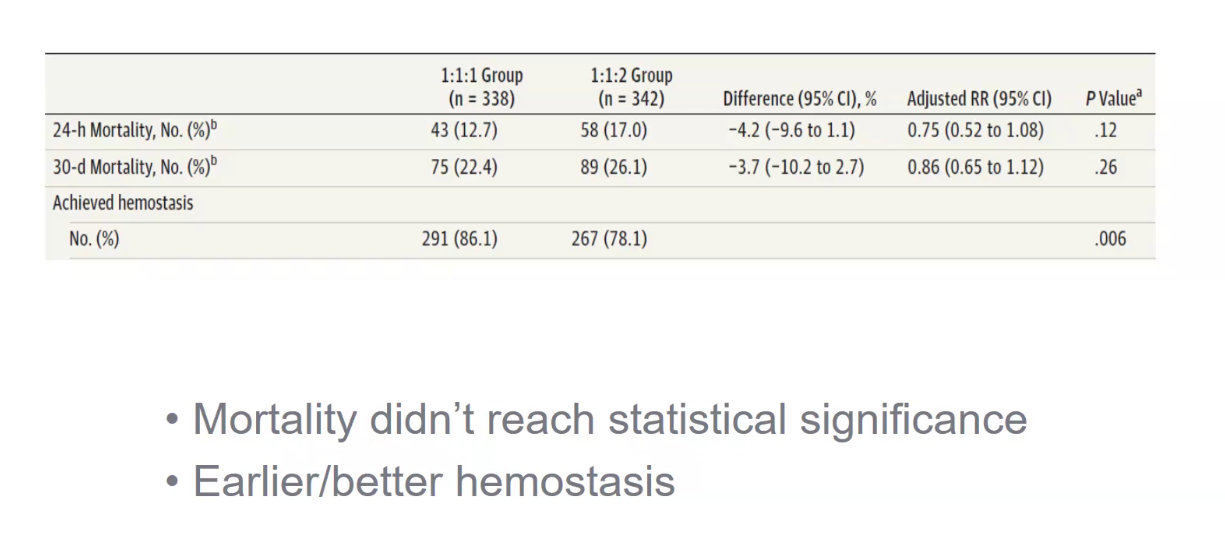
- very big study
Combat:
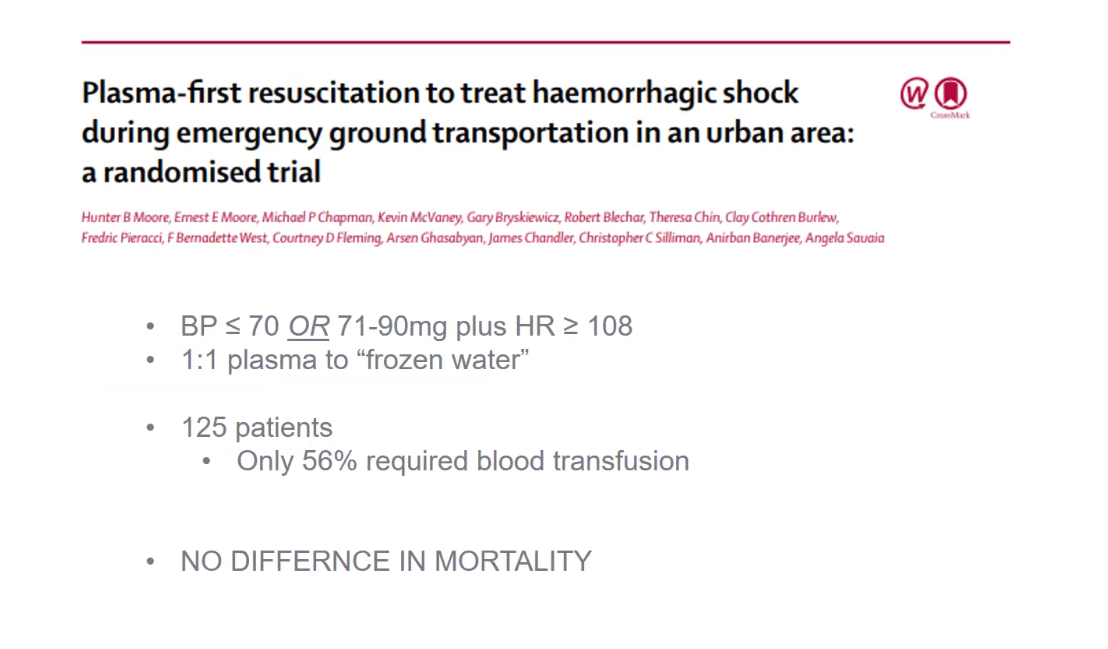
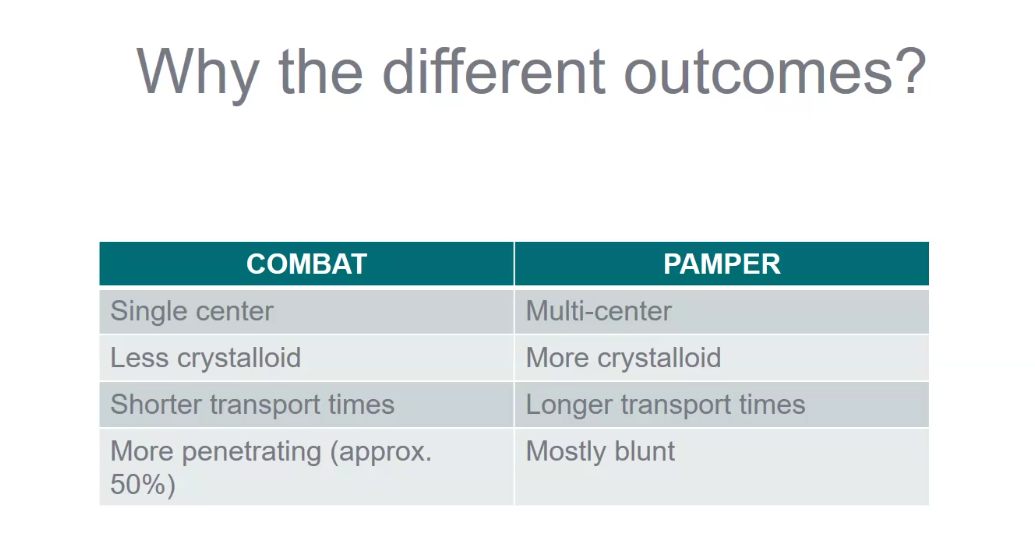
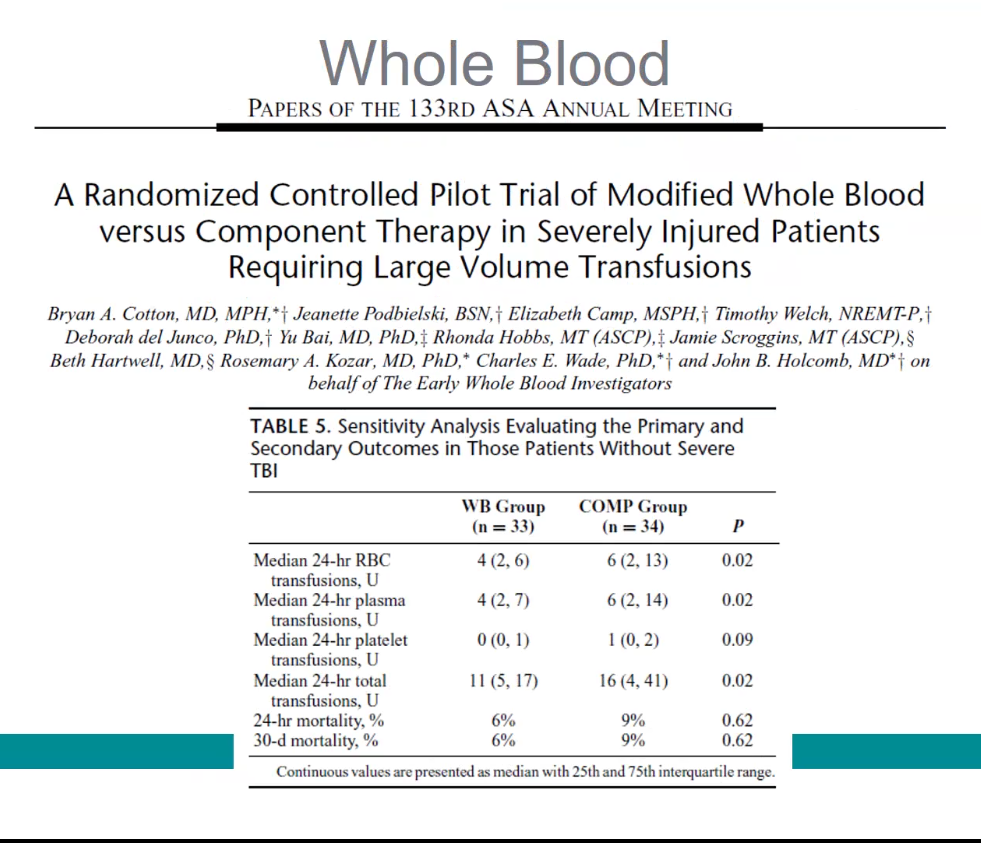
- secondary analysis showed whole blood did better
- 2 reasons switched to component:
- easier to store component therapy
- whole blood: can make more money with different components
- severe TBI excluded
- massive improvement with whole blood
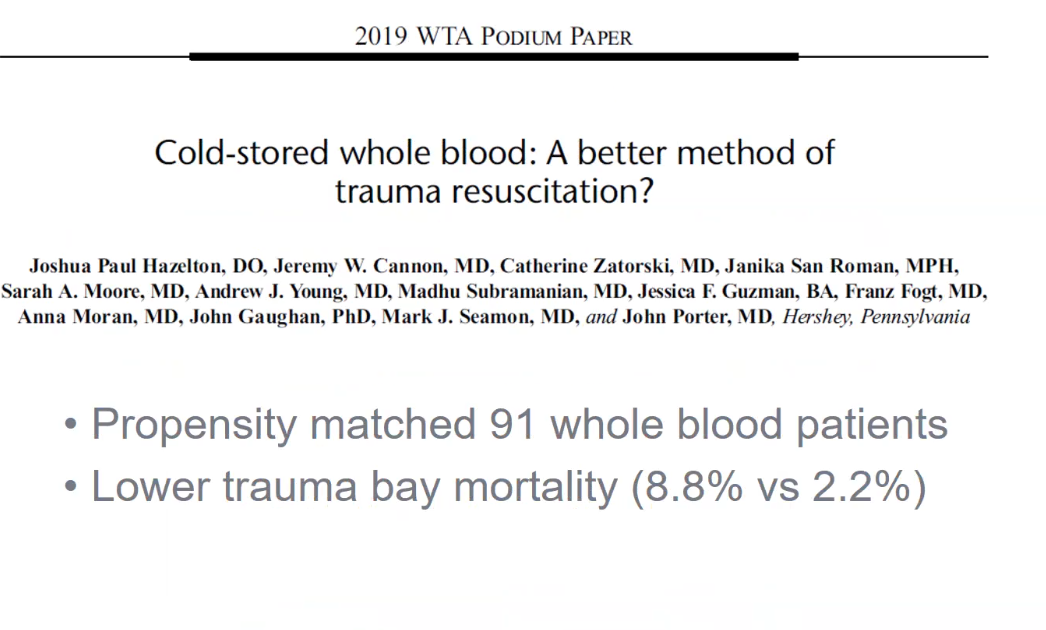
- trauma bay mortality not really helpful
- no real data to support whole blood being better
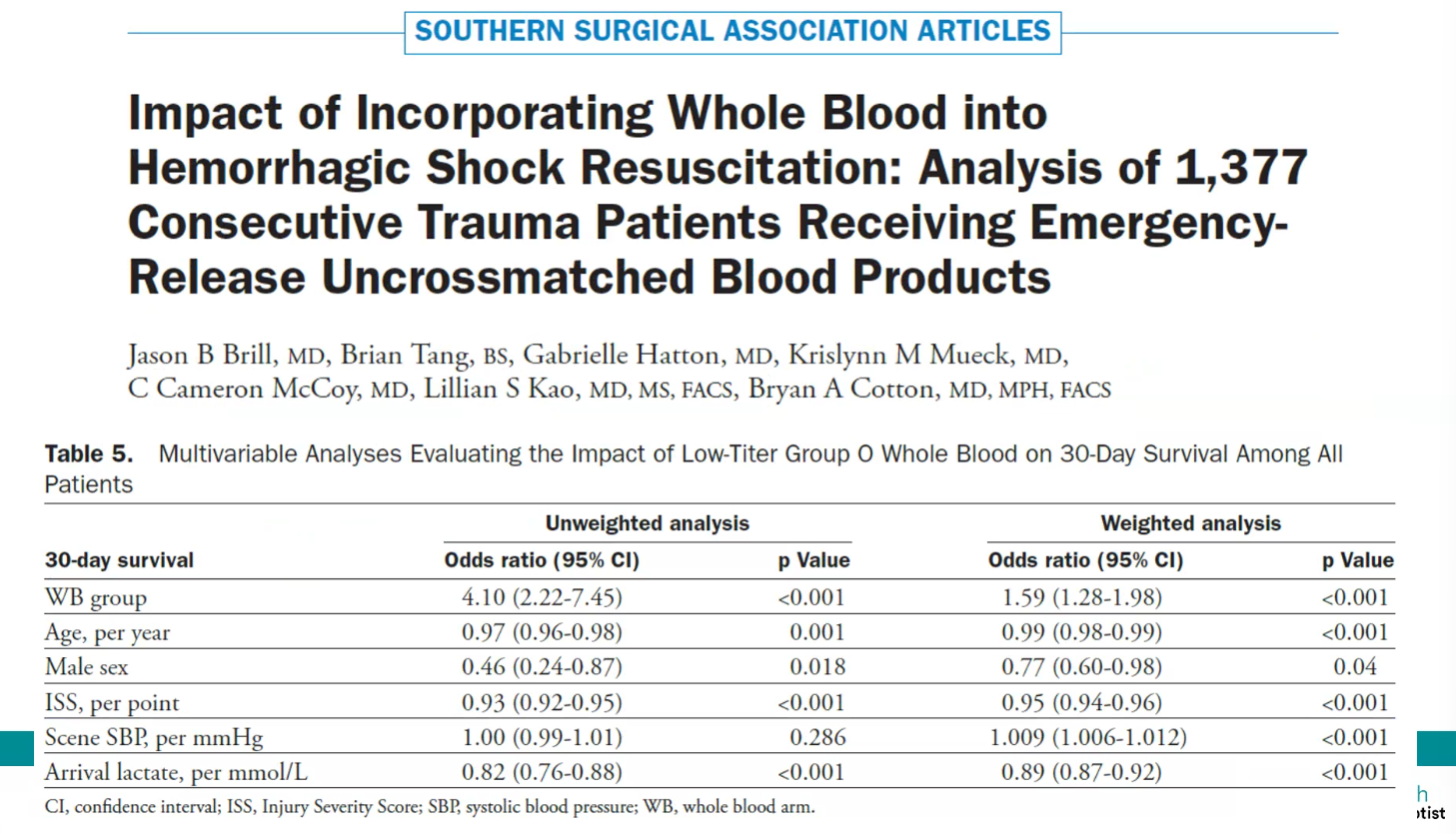
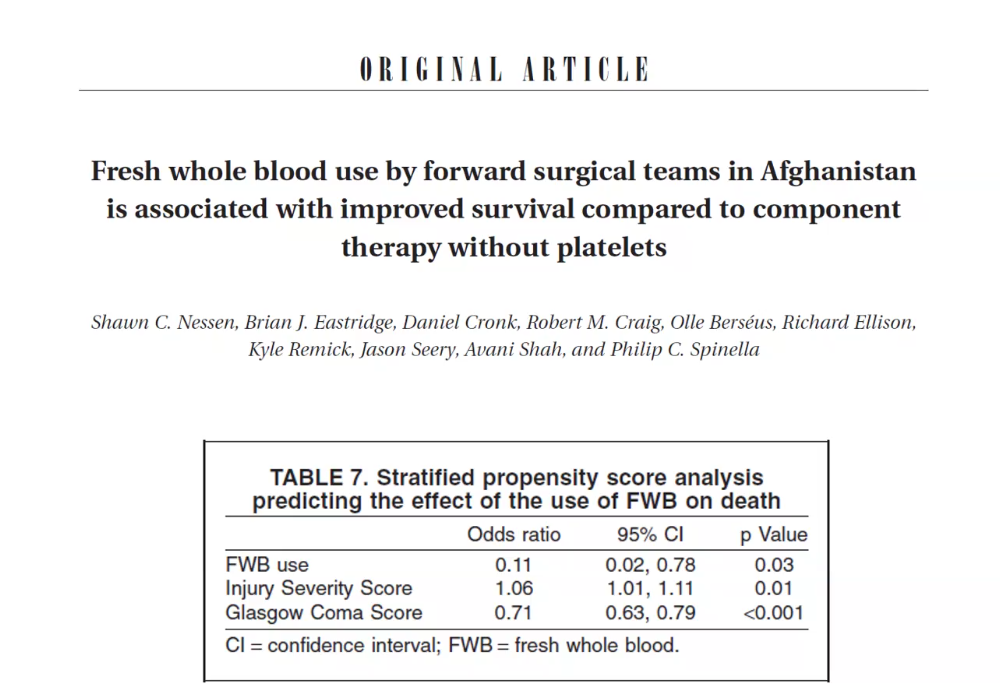
- odds survival much better in whole blood
- still not convincing

- current trial
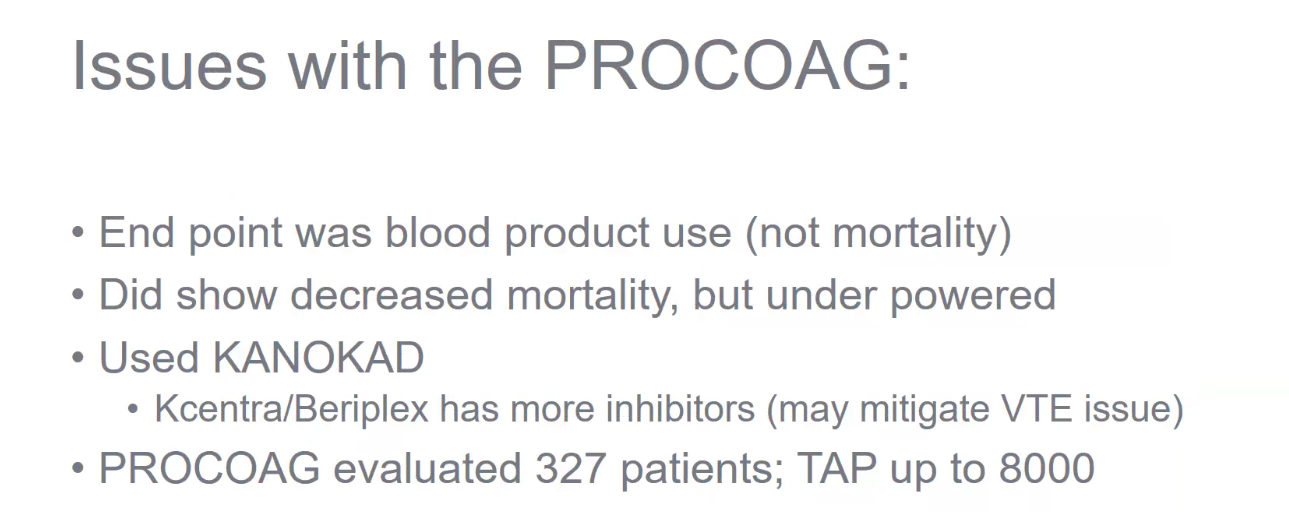
PCC
- AKA Kcentra
- 1 dose 2,000u
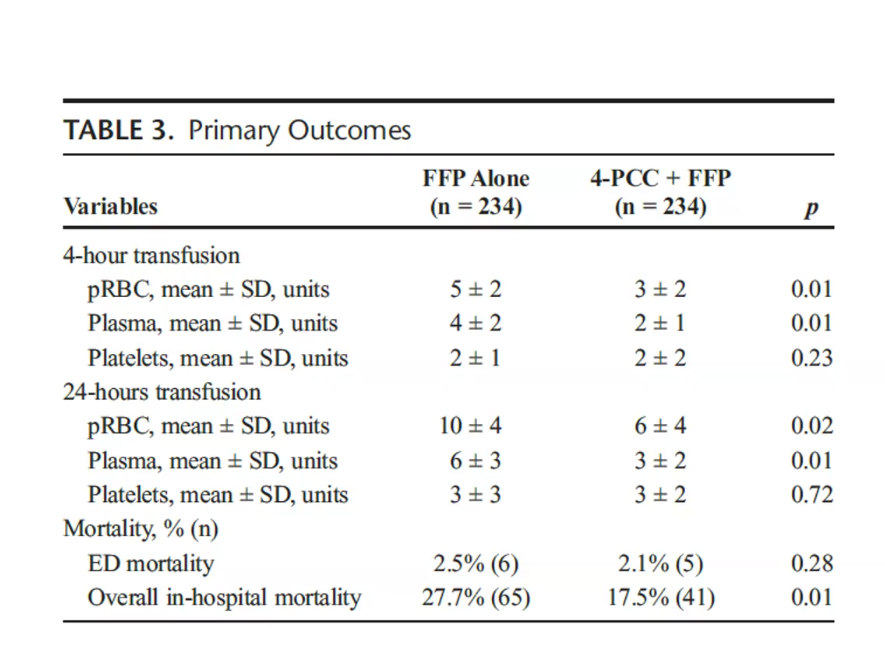
- FFP with PCC better
- no difference in mortality
- difference in VTE
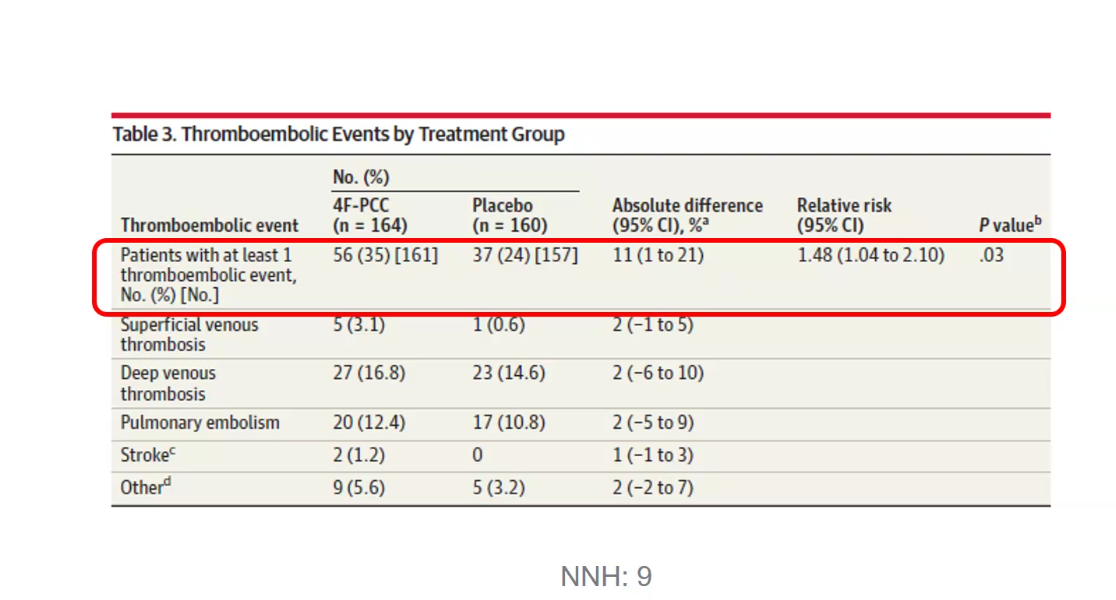
Current trial:
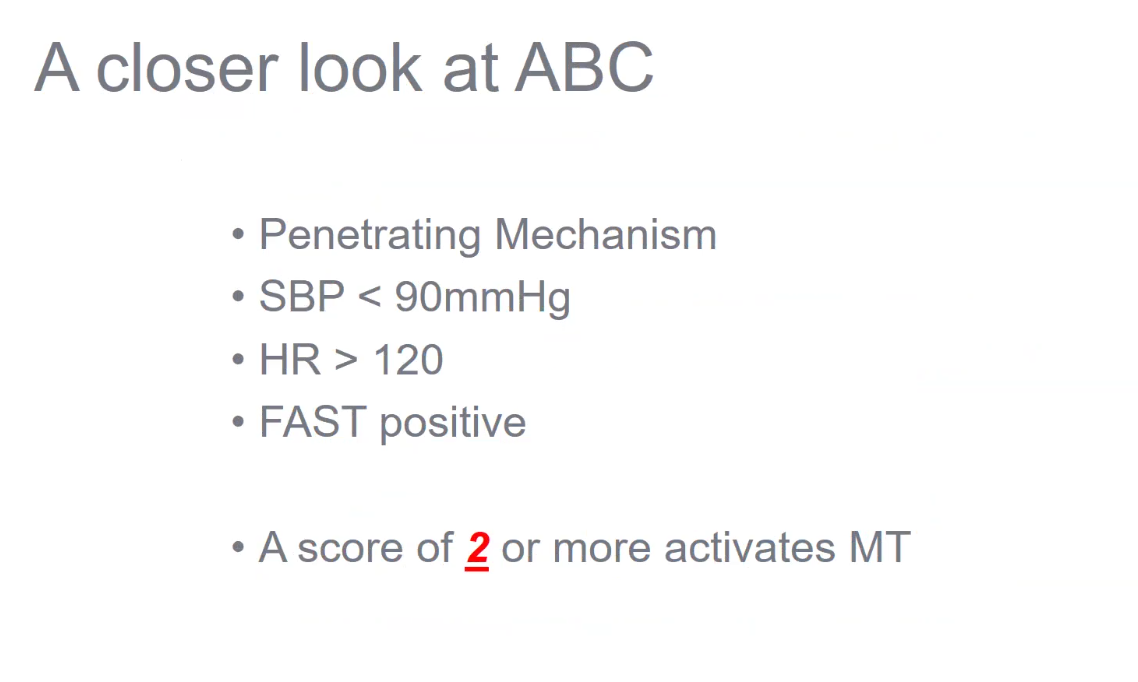
When to activate MTP
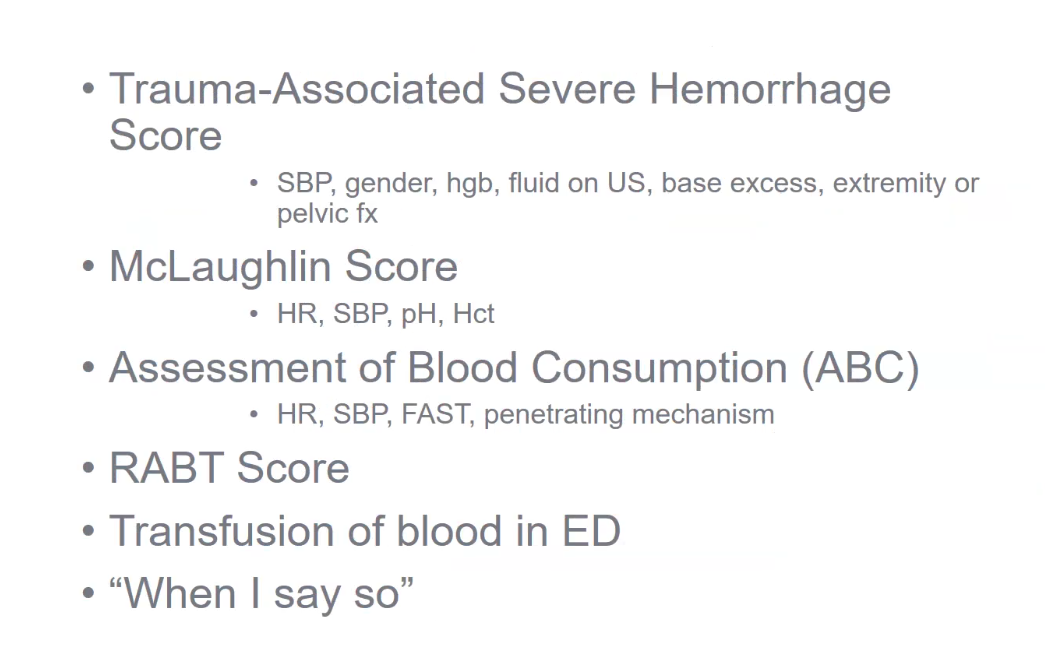
- first 2: needs labs
- FFP: liquid plasma is used more at Wake (can return)
- not really used anymore
- plt: aphresis. Here 1:1:1 at Wake.
- vasopressin for MTP? AVERT trial