treatment for elevated ICP includes hypertonic saline and mannitol
- related: intracranial pressure ICP and cerebral perfusion pressure goals and treatment in TBI, traumatic brain injury overview
- tags: #permanent
General considerations:
- Avoid hyperthermia
- Hyperventilation is not supported
- Steroids is not supported
- Paralytics is not recommended: use normal pain/sedation regimen (propofol/versed for intubated patients, barbiturates/Precedex for non)
- Use seizure prophylaxis for 7 days
- Beta blocker to avoid neuro storm, anxiety
Medical treatment for elevated ICP involves either hypertonic saline or mannitol. Start with hypertonic saline then proceeds to mannitol once you hit targeted serum sodium and still has elevated ICP.
Hypertonic Saline
- Give hypertonic saline for patients with elevated ICP (intracranial pressure ICP and cerebral perfusion pressure goals and treatment in TBI)
- Use “bullet,” 23.4% NaCl bolus after consultation with NSY. Can only be used centrally
- Use 3% hypertonic saline normally
- bolus: 3% 250cc over 30 minutes, can be given once peripherally emergently
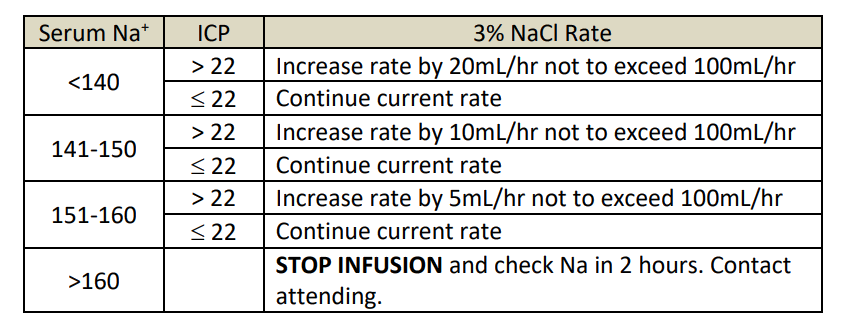
- infusion: use 3% up to 50cc/hr per IV for up to 100cc total, otherwise give centrally
- Check BMP every 4 hours
- Deescalate by half the infusion rate and then discontinue if no change in ICP
- Titration guideline:
Mannitol
- use for elevated, sustained ICP
- 0.25 - 1 gm/kg (e.g. 70 gm for 70 kg) once every q6h PRN
- Maintain serum osm ≤ 320. Calculate osmolar gap if serum osm > 320
- Don’t use if osmolar gap > 20 use osmolar gap for mannitol administration for hypernatremia
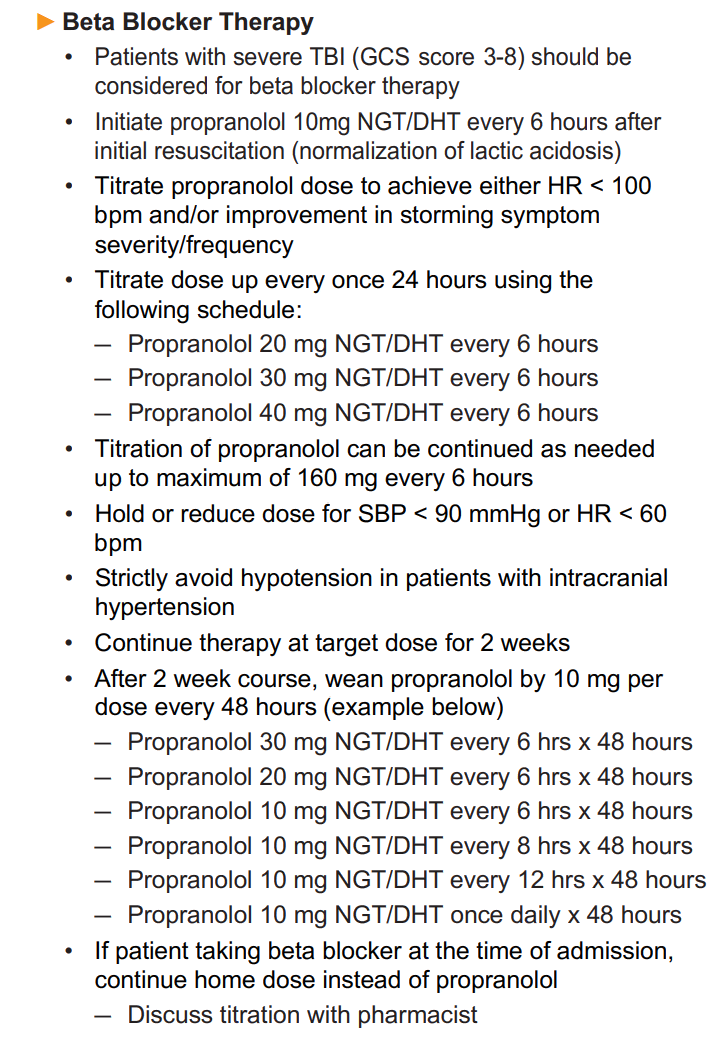
Beta Blocker
- beta blocker has neuroprotective effects
- decreases cerebral metabolism, O2 and glucose consumption
- reduces sympathetic activity that comes with TBI. These includes tachycardia, hypertension, tachypnea, hyperthermia
- can be cardioprotective by avoiding increased myocardial O2 consumption1
Links to this note
-
intracranial pressure ICP and cerebral perfusion pressure goals and treatment in TBI
- The goal for ICP is less than 22. Treatment is often initiated for patients with ICP greater than 22. treatment for elevated ICP includes hypertonic saline and mannitol is discussed separately.