accelerated idioventricular rhythm AIVR after STEMI
- related: Cardiology and Hemodynamics
- tags: #literature #cardiology
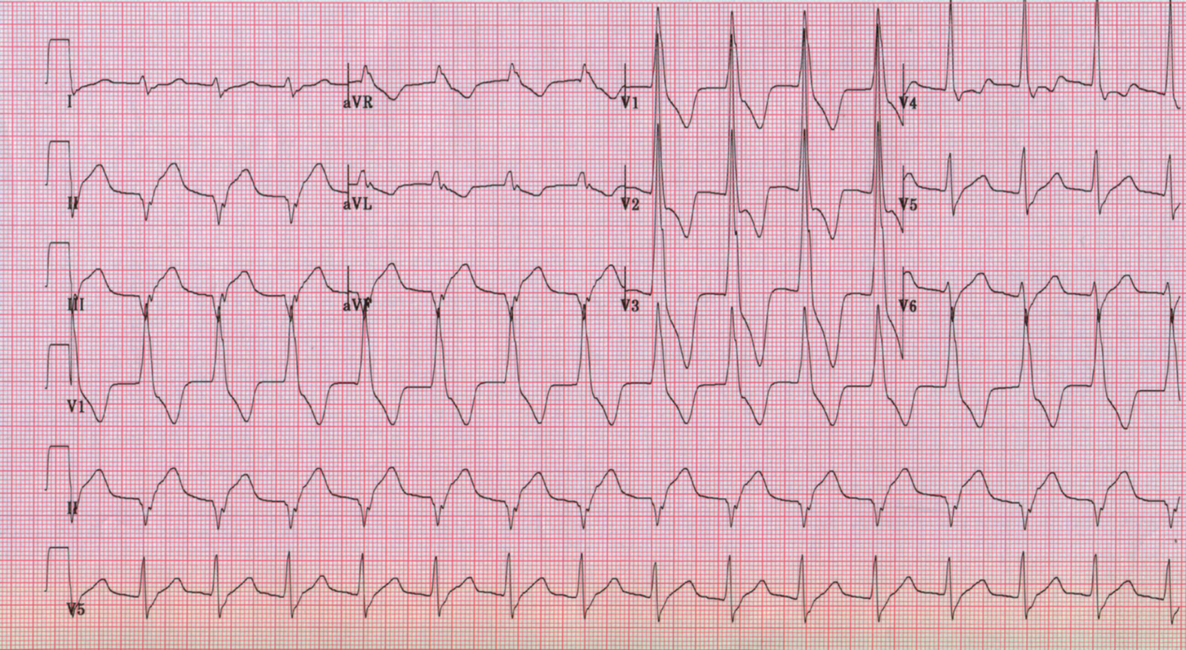
The ECG reveals accelerated idioventricular rhythm (AIVR). In the setting of acute infarction, this is a reperfusion arrhythmia and probably results from increased automaticity of Purkinje fibers. AIVR is relatively specific but not entirely sensitive for patency of the infarct-related artery. The rate of AIVR is generally from 60 to 100/min (as opposed to ventricular escape rhythms, which run from 30 to 50/min). Ventricular rates greater than 100/min are termed ventricular tachycardia. Because the rhythm is usually transient and this heart rate is well tolerated, it is rarely necessary to treat AIVR; observation will usually suffice. AIVR is not associated with sustained ventricular tachycardia, ventricular fibrillation, or a worse prognosis. Reperfusion is sometimes associated with ventricular rhythms at rates greater than 100/min but less than 120/min (“slow VT”). If these rhythms are transient and well tolerated, they may be observed as well. Faster ventricular rhythms, and those not well tolerated hemodynamically, should be treated like ventricular tachycardia.
In this question, continuing the heparin implies observation of the cardiac rhythm without specific treatment. Heparin is generally continued for 24 h after percutaneous coronary intervention for acute myocardial infarction. The patient is clinically stable and has evidence of reperfusion. There is no reason to perform cardioversion and also no reason to attempt to suppress the rhythm with lidocaine or amiodarone. Even though the rhythm is not sinus, it is stable, and there is no symptomatic bradycardia, so temporary pacing is unnecessary. 123