CAR-T and cytokine release syndrome
- related: Oncology
- tags: #literature #hemeonc
- host immune system activated to attack underlying cancer
- ICANS: CNS mediated inflammatory response
- most important: identify patients who need early therapy
- simple criteria: fever, hypotension, hypoxemia
- ICANS: steroid very effective
- as you suppress immune system, you make CAR-T less likely to work. Consult oncology early.1
CRS is the most common serious toxicity of CAR-T therapy. It is an acute systemic inflammatory response elicited by proinflammatory cytokines released from CAR-T cells that are activated after they have encountered tumor cells. The diagnosis of CRS is made clinically in the correct clinical setting of fever, with or without hypotension, hypoxia, and/or other end-organ dysfunction. Treatment for mild CRS includes supportive care. For more severe CRS cases, such as those in patients with stage 3 or 4 disease and/or requiring admission to the ICU, as in this case, tocilizumab, a monoclonal antibody against the IL-6 receptor, is recommended; for very severe cases, addition of corticosteroids is often recommended. Supportive care alone is insufficient. Despite the often difficult therapeutic course, in general, CRS associated with CAR-T therapy has a good prognosis with treatment.
The differential diagnosis for CRS is broad and includes sepsis, tumor lysis syndrome (TLS), left ventricular dysfunction, heart failure, pulmonary VTE, drug reactions, and disease progression. Although bacteremia can occur in 10% to 30% of patients treated with CAR-T therapy, this patient is on appropriate bacterial coverage for sepsis, they are not absolutely neutropenic, procalcitonin level is normal, 1,3-β-D-glucan and galactomannan tests are negative, and the event is temporally related to the CAR-T therapy; therefore, ongoing sepsis is less likely. The patient is on allopurinol and at medium risk for TLS; nevertheless, even though many laboratories are suggesting that TLS be defined by levels of hyperuricemia, hyperkalemia, hyperphosphatemia, and hypocalcemia, this patient does not meet the standard definition of TLS. In this case, lower extremity venous ultrasound studies are negative, the patient is thrombocytopenic, and they have been on prophylactic heparin; hence, even though the D-dimer value is elevated, it is also an acute phase reactant, so diagnosis of pulmonary embolism is less likely. In addition, bedside point-of-care ultrasound did not note elevated right-sided pressures, and brain-type natriuretic peptide level is only mildly elevated.
This patient has developed cytokine release syndrome (CRS) from the CAR-T cell therapy administered for lymphoma, and tocilizumab should be started (choice C is correct). CAR-T cell therapy is indicated in relapsed and refractory lymphoma, acute lymphoblastic leukemia, and multiple myeloma, among other malignancies. The therapy is associated with high response rates, long-term remissions, and potential for cure but is associated with multiple, severe, potentially life-threatening but also reversible side effects. In most series, 10% to 47% of patients will develop severe toxicities with severe organ dysfunction, and a large proportion of these patients require ICU care, including fluid therapy, vasoactive drugs for BP support, invasive or noninvasive mechanical ventilation, and/or renal replacement therapy. The most common serious CAR-T cell side effects include CRS, as in this case, which develops in 37% to 93% of cases. Immune effector cell-associated neurotoxicity syndrome develops in 23% to 67%, sepsis in 8% to 16%, and B-cell aplasia/hypogammaglobulinemia in 56% to 88%. Multiple toxicities can develop in the same patient. CRS severity may be related to the underlying tumor type and burden, the agent chosen, and the dose of agent. Axicabtagene ciloleucel is a highly effective CAR-T cell treatment for relapsed and refractory aggressive B-cell lymphoma. It is complicated by the occurrence of CRS in more than 90% of patients.
CRS is the most common serious toxicity of CAR-T cell therapy. It is an acute systemic inflammatory response elicited by proinflammatory cytokines released from CAR-T cells that are activated after they have encountered tumor cells. The initial reaction activates other cells, including macrophages, endothelial cells, and stromal cells, resulting in further proinflammatory cytokine release and cytokine storm. IL-6 is one of the key driving cytokines in CRS. Others include IL-8, IL-10, and interferon γ.
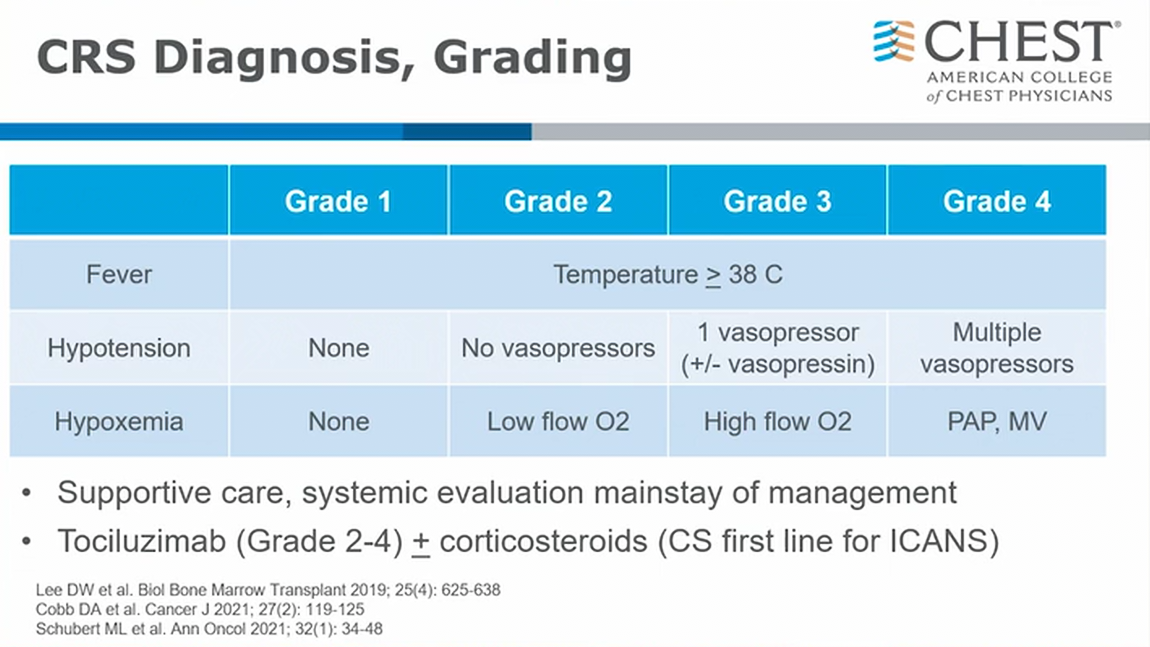
CRS is diagnosed clinically in the correct clinical setting with fever, with or without hypotension, hypoxia, and/or other end-organ dysfunction. CRS usually develops within hours to days (2-3 days, up to 58 days) after treatment with a drug in this class, but the timing can vary. Clinically, CRS is characterized by fever (≥38.0 °C), hypoxemia, and hypotension and, in severe cases, circulatory shock and multiple organ dysfunction. Mild CRS disease is characterized by flu-like symptoms, fever, fatigue, headache, rash, diarrhea, arthralgias, and myalgias. In severe CRS, the fever may be high, and patients may have hypotension and circulatory collapse, vascular leak, peripheral and/or pulmonary edema, renal failure, cardiac dysfunction, and multiorgan system failure. CRS is graded from 1 to 4. Recipients in stages 3 and 4 who are affected are treated in the ICU. All patients with CRS have fever, and the severity grade is based on requirements for vasopressor and respiratory support.
Laboratory abnormalities include hypophosphatemia or hyperphosphatemia, hypokalemia or hyperkalemia, and hyponatremia. Renal insufficiency is common. Often leukocyte abnormalities and thrombocytopenia are common and may relate to other chemotherapeutic agents, lymphodepleting chemotherapy, the underlying malignancy, and/or subsequent treatment. It is not uncommon for activated or abnormal lymphocytes to be seen on the peripheral blood smear after CAR-T cell therapy. Abnormalities in renal or liver function test results are common. Levels of nonspecific inflammatory markers, including C-reactive protein (CRP) and ferritin, are always elevated in CRS. Levels of inflammatory cytokines such as IL-6, IL-10, and soluble IL-2R-α are also elevated. Laboratory test results suggestive of tumor lysis syndrome (TLS) can be seen and include hyperuricemia, hyperkalemia, hyperphosphatemia, and hypocalcemia. In general, the degree of elevation of cytokines and markers of inflammation correlate with the severity of the clinical syndrome. Marked elevation of IL-6 is a supportive finding for the diagnosis of CRS. CRP is not specific for CRS and is not as useful for clinical monitoring, especially after tocilizumab is administered.
Treatment for mild CRS includes supportive care. For more severe CRS cases, such as those in patients with stage 3 or 4 disease, and those requiring admission to the ICU as in this case, tocilizumab, a monoclonal antibody against the IL-6 receptor, is recommended. For very severe cases, the addition of corticosteroids is often recommended. Supportive care alone is insufficient (choice D is incorrect). Tocilizumab can mask fevers and signs of infection, so a high index of suspicion for infection should remain. The concern with corticosteroids used alone, too early, and when not absolutely needed, is that they can compromise the activity of the CAR-T cells. Higher doses or prolonged glucocorticoid therapy may deplete or eradicate CAR-T cells. Despite the often difficult therapeutic course, in general, CRS associated with CAR-T cell therapy has a good prognosis with treatment.
The differential diagnosis for CRS is broad and includes sepsis, TLS, left ventricular dysfunction, heart failure, pulmonary venous thromboembolism, drug reactions, and disease progression. In this case, the bedside point-of-care ultrasound has helped eliminate some of these diagnoses. Although bacteremia can occur in 10% to 30% of patients treated with CAR-T cell therapy, this patient is receiving appropriate bacterial coverage for sepsis, is not absolutely neutropenic, has normal procalcitonin levels, and has negative test results for 1,3-β-D-glucan and galactomannan, and the event is temporally related to the CAR-T cell therapy, so voriconazole should not yet be added to the regimen (choice B is incorrect). The patient is receiving allopurinol, and although is at medium risk for TLS and has many laboratory test results suggesting TLS (defined by levels of hyperuricemia, hyperkalemia, hyperphosphatemia, and hypocalcemia), this patient does not meet the standard definition for TLS, and rasburicase is likely not needed (choice A is incorrect). In this case, lower extremity venous ultrasonographic studies are negative, the patient is thrombocytopenic and has been receiving prophylactic heparin, and although the D-dimer level is elevated, it is also an acute phase reactant, and thus a diagnosis of pulmonary embolism is less likely. In addition, the bedside point-of-care ultrasound did not indicate elevated right-sided pressures, and the brain-type natriuretic peptide level is only mildly elevated.234567
Links to this note
-
invasive pulmonary aspergillosis
- The most rapidly progressive and lethal consequence of exposure to Aspergillus spores is invasive aspergillosis, which occurs in patients who are immunosuppressed, with the lung the most commonly recognized site of infection, although dissemination via circulation can occur. Typical settings include patients who are neutropenic undergoing bone marrow transplant, solid organ transplant recipients, and patients undergoing CAR-T cell therapy, especially if it has been complicated by cytokine release syndrome, which requires treatment with tocilizumab and corticosteroids (CAR-T and cytokine release syndrome), as in the patient presented. Invasive aspergillosis has also been described in patients with advanced cirrhosis and after prolonged courses of respiratory failure managed with mechanical ventilation in the ICU, including COVID-19 pneumonitis.
-
CAR-T and ICANS immune effector cell associated neurotoxicity syndrome
- related: Oncology, CAR-T and cytokine release syndrome
Footnotes
-
Azoulay É, Castro P, Maamar A, et al; Nine-I investigators. Outcomes in patients treated with chimeric antigen receptor T-cell therapy who were admitted to intensive care (CARTTAS): an international, multicentre, observational cohort study. Lancet Haematol. 2021;8(5):e355-e364. PubMed ↩
-
Jones GL, Will A, Jackson GH, et al; British Committee for Standards in Haematology. Guidelines for the management of tumour lysis syndrome in adults and children with haematological malignancies on behalf of the British Committee for Standards in Haematology. Br J Haematol. 2015;169(5):661-671. PubMed ↩
-
Outcomes in patients requiring intensive care for CAR T-cell toxicity. Drug Ther Bull. 2021;59(11):166. PubMed ↩
-
Shimabukuro-Vornhagen A, Böll B, Schellongowski P, et al. Critical care management of chimeric antigen receptor T-cell therapy recipients. CA Cancer J Clin. 2022;72(1):78-93. PubMed ↩
-
Yan Z, Zhang H, Cao J, et al. Characteristics and risk factors of cytokine release syndrome in chimeric antigen receptor T cell treatment. Front Immunol. 2021;12:611366. PubMed ↩